Bipolar Disorder Symptoms: A Complete Guide to Mania, Hypomania, and Depression
Sixty-nine percent of people with bipolar disorder are initially misdiagnosed. Most walk into a psychiatrist’s office during a depressive episode, never mentioning the week last spring when they felt invincible, slept three hours a night, and started two businesses.
The clinician writes a prescription for major depression, and the real story stays hidden for years—sometimes a decade.
Understanding bipolar disorder symptoms isn’t just about memorizing a checklist from the DSM-5. It’s about recognizing your polarity pattern, learning your earliest warning sign, and building cycle awareness before treatment selection. Because here’s what decades of clinical data show: the right med for the wrong cycle can destabilize you faster than no medication at all.
This guide walks you through what mania, hypomania, and depression actually feel like in your body and brain, how symptoms vary across bipolar I, II, and cyclothymic disorder, and why mixed features—when highs and lows overlap—carry the highest suicide risk.
You’ll learn to match the intervention to your episode and start building a mood tracking inventory that protects your sleep architecture and nervous system regulation.
Key Takeaways
- Manic episodes require seven days of elevated mood plus three specific symptoms (or four if you’re only irritable), while hypomanic episodes need just four days with no major impairment—the distinction determines your diagnosis and treatment protocol.
- Most people with bipolar disorder first seek help during depression, not mania, which explains the 69% misdiagnosis rate and why hypomania often goes unreported until a crisis hits.
- Mixed features—experiencing symptoms of both poles simultaneously—occur in up to 33% of episodes and carry the highest suicide risk, especially when agitation meets hopelessness.
- Bipolar II patients spend significantly more time depressed than those with bipolar I, yet their suicide risk equals or exceeds it, making accurate subtype identification critical for sustainable stability.
- Tracking your true baseline between episodes reveals residual symptoms that predict the next cycle, giving you a trigger-and-response map before mood destabilization begins.
What Are the Symptoms of Bipolar Disorder?
Bipolar disorder symptoms fall into three main categories: manic episodes, hypomanic episodes, and depressive episodes. Some people experience mixed features, where symptoms from opposite poles show up at the same time. Between episodes, you might notice residual symptoms that never fully resolve.
The key isn’t just identifying symptoms in isolation. It’s recognizing your polarity pattern—whether you cycle more toward mania or depression, how long episodes last, and what triggers the shift. That pattern determines everything from medication selection to lifestyle interventions.
Your symptoms also depend on which type of bipolar disorder you have. Bipolar I disorder requires at least one full manic episode. Bipolar II involves hypomanic episodes plus major depression. Cyclothymic disorder shows chronic fluctuation between mild highs and lows that never meet full episode criteria.
Manic Episode Symptoms
What Mania Feels Like
Mania feels like your brain’s reward circuitry gets stuck holding down the accelerator. Your thoughts race so fast you can’t finish sentences. You feel invincible, like you’ve unlocked a secret level of human capability that everyone else is too timid to access.
Sleep becomes optional—not because you’re forcing yourself awake, but because your body genuinely doesn’t need it. Three hours feels like eight. You wake up buzzing with energy, ready to execute the five projects you started yesterday and the three new ones that just occurred to you.
Your speech speeds up to match your thoughts. You interrupt constantly because waiting for someone to finish feels physically painful. Ideas cascade so quickly that you jump from topic to topic, leaving others confused about how you got from discussing dinner plans to explaining your theory about quantum consciousness.
Common manic symptoms include:
- Elevated or irritable mood that feels distinctly different from your baseline
- Decreased need for sleep without feeling tired (not insomnia—you genuinely don’t want to sleep)
- Racing thoughts that feel like ten browser tabs open simultaneously
- Increased goal-directed activity or physical restlessness
- Excessive talking or pressure to keep speaking
- Inflated self-esteem or grandiosity (believing you have special powers, connections, or abilities)
- Distractibility where every stimulus pulls your attention
- Increased risky behavior (spending sprees, sexual indiscretions, reckless driving, impulsive business decisions)
Where Mania Crosses Into Danger
Mania becomes dangerous when your judgment collapses completely. You drain your bank account on a business idea you conceived three hours ago. You drive 90 mph because you’re convinced you have supernatural reflexes. You stop your bipolar disorder medications because you’ve decided you were misdiagnosed and you’re actually just more evolved than other people.
Psychotic features can emerge during severe mania. You might develop delusions—fixed false beliefs that feel absolutely true, like believing you’re being monitored by the government or that you’ve been chosen for a special mission. Hallucinations are less common but possible, usually auditory.
The irritability during mania gets underestimated. You’re not just annoyed—you’re enraged when anyone questions your plans or tries to slow you down. That rage can escalate to verbal or physical aggression, especially when combined with impaired judgment and reduced impulse control.
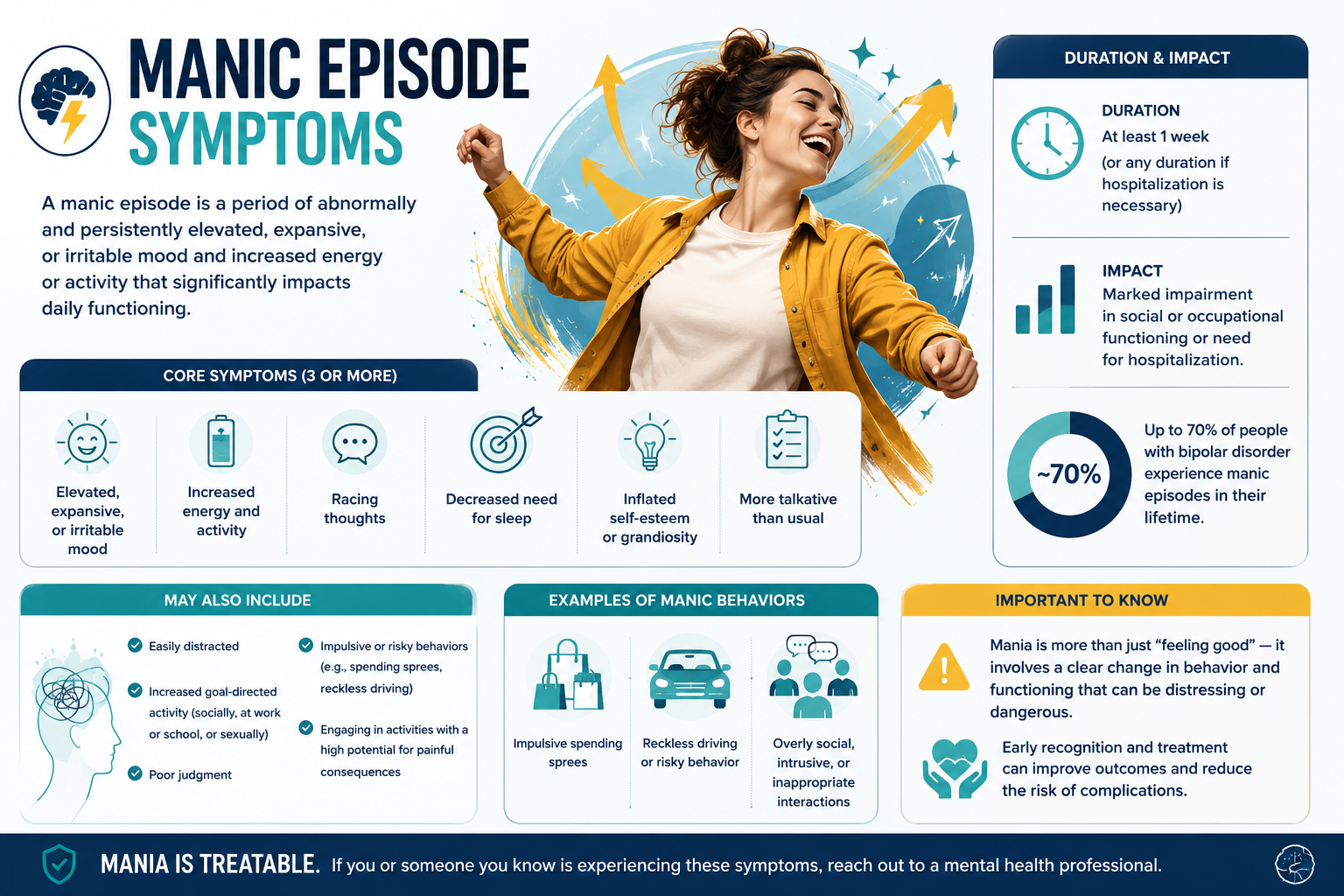
DSM-5 Diagnostic Criteria for a Manic Episode
The DSM-5 requires a distinct period of abnormally elevated, expansive, or irritable mood plus increased energy or activity lasting at least seven days (or any duration if hospitalization is required). During that period, you need three or more of these symptoms (four if your mood is only irritable, not elevated):
- Inflated self-esteem or grandiosity
- Decreased need for sleep
- More talkative than usual or pressure to keep talking
- Racing thoughts or flight of ideas
- Distractibility
- Increase in goal-directed activity or psychomotor agitation
- Excessive involvement in risky activities
The episode must cause marked impairment in social or occupational functioning, require hospitalization, or include psychotic features. It can’t be due to substances or another medical condition.
That “marked impairment” threshold matters. If you’re still functioning at work and maintaining relationships, it’s probably hypomania, not mania—even if you feel absolutely terrible.
Hypomanic Episode Symptoms
Hypomania uses the same symptom list as mania but with lower intensity and shorter duration. You need at least four consecutive days of elevated or irritable mood plus three symptoms (four if only irritable). The crucial difference: no marked impairment, no hospitalization, and no psychotic features.
Hypomania often feels good—sometimes better than your true baseline. You’re productive, creative, socially confident, and energized. You get more done in a week than you usually accomplish in a month. Your friends comment on how great you seem.
That’s exactly why hypomania goes unreported. When you finally see a psychiatrist during a depressive crash, you don’t mention the “good weeks” because they didn’t feel like symptoms. They felt like finally being yourself.
But hypomania still carries risk. The decreased need for sleep disrupts your sleep architecture, setting up the next depressive episode. The increased activity and goal-directed behavior can lead to overcommitment. The elevated mood can shift into irritability or escalate into full mania, especially if you’re taking antidepressants without a mood stabilizer.
Hypomania warning signs to track:
- Needing less sleep but feeling energized (not tired and wired)
- Starting multiple projects with intense enthusiasm
- Increased talkativeness or social engagement
- Feeling unusually confident or capable
- Mild increase in risky behavior (overspending, impulsive decisions)
- Irritability when interrupted or contradicted
The challenge with hypomania in bipolar II disorder is that it’s often brief and pleasant, making it easy to dismiss. But tracking these episodes is essential for accurate diagnosis and treatment planning.

Depressive Episode Symptoms
Emotional Symptoms
Bipolar depression feels different from sadness. It’s a physical heaviness that makes your limbs feel like they’re filled with concrete. Your brain slows down—thoughts become sluggish, decisions feel impossible, and concentrating on anything requires exhausting effort.
The emotional numbness surprises people. You’re not crying all the time. You’re not feeling much of anything. Activities that used to bring joy—seeing friends, listening to music, eating your favorite food—produce nothing. That absence of feeling is its own kind of suffering.
Hopelessness in bipolar depression has a particular quality. It’s not just “things are bad right now.” It’s “things have always been bad, will always be bad, and I was delusional to ever think otherwise.” Your brain rewrites your entire history through a lens of failure and futility.
Core emotional symptoms include:
- Persistent sad, empty, or hopeless mood lasting most of the day, nearly every day
- Loss of interest or pleasure in activities you normally enjoy (anhedonia)
- Feelings of worthlessness or excessive guilt about past events or current circumstances
- Difficulty concentrating, remembering, or making decisions
- Recurrent thoughts of death or suicide (not just fear of dying, but active ideation)
Physical and Behavioral Symptoms
The physical symptoms of bipolar depression often dominate. You might sleep 12-14 hours and still wake up exhausted. Or you might develop insomnia, lying awake for hours with your mind cycling through every mistake you’ve ever made.
Appetite changes go both directions. Some people lose all interest in food and drop weight rapidly. Others experience increased appetite and carbohydrate cravings, gaining weight that then feeds into feelings of worthlessness and loss of control.
Psychomotor changes become visible to others. You might move and speak slowly, with long pauses before responding. Or you might experience agitation—pacing, hand-wringing, inability to sit still—while simultaneously feeling exhausted.
Physical and behavioral symptoms include:
- Sleep disturbances (hypersomnia is more common in bipolar depression than in unipolar depression)
- Appetite or weight changes (increase or decrease)
- Fatigue or loss of energy nearly every day
- Psychomotor agitation or retardation observable by others
- Physical aches and pains without clear medical cause
- Withdrawal from social activities and relationships
Why Bipolar Depression Gets Missed
Bipolar depression gets misdiagnosed as major depressive disorder because most people seek help during depressive episodes, not manic or hypomanic ones. You walk into the psychiatrist’s office feeling suicidal, and the immediate priority is addressing that crisis. The clinician asks about depression symptoms, you confirm them all, and you walk out with an antidepressant prescription.
The problem: antidepressants without mood stabilizers can trigger mania or rapid cycling in up to 25% of people with bipolar disorder. That’s why cycle awareness before treatment selection matters so much. If you can report even brief periods of elevated mood, decreased sleep need, or increased energy, it changes the entire treatment approach.
Hypersomnia and increased appetite are more common in bipolar depression than unipolar depression, but they’re subtle clues that often get overlooked. If you’re sleeping 12 hours a day and still exhausted, that pattern suggests bipolar depression over major depressive disorder.
The diagnosis process requires a careful history that includes questions about past periods of elevated mood, even if they felt good at the time. That’s why bringing a mood tracking inventory to your first appointment can be transformative.
Mixed Features: When Highs and Lows Overlap
Mixed features occur when you experience symptoms from both poles simultaneously during a manic, hypomanic, or depressive episode. You might feel depressed and hopeless while also experiencing racing thoughts and agitation. Or you might feel euphoric and energized while simultaneously having suicidal thoughts.
The DSM-5 added a “mixed features specifier” because pure-pole episodes are actually less common than we thought. Up to 33% of episodes in real-world populations include mixed features, especially in younger adults.
Mixed states carry the highest suicide risk of any bipolar presentation. When you combine the hopelessness and suicidal ideation of depression with the energy and impulsivity of mania, you get a lethal combination. Research shows that hypomania with mixed features has an odds ratio of 29.43 for suicidal ideation compared to pure hypomania.
Common mixed feature presentations:
- Agitated depression: profound sadness plus racing thoughts, restlessness, and irritability
- Dysphoric mania: elevated mood plus feelings of worthlessness, guilt, or suicidal thoughts
- Anxious mania: euphoria plus severe anxiety and panic symptoms
- Irritable mixed state: intense irritability plus both depressive and manic symptoms
The agitation component is what makes mixed states so dangerous. You have the despair that makes you want to die plus the energy and impulsivity to act on it. That’s why recognizing mixed features early and adjusting treatment immediately is critical for safety.
Treatment for mixed features typically requires mood stabilizers or atypical antipsychotics rather than antidepressants, which can worsen the mixed state. The side-effect trade-off becomes worth it when you’re comparing sedation or weight gain against suicide risk.
How Symptoms Vary by Type
Bipolar I Disorder Symptoms
Bipolar I requires at least one manic episode lasting seven days or requiring hospitalization. You might also experience hypomanic and depressive episodes, but they’re not required for diagnosis. The manic episode is the defining feature.
People with bipolar I often experience psychotic features during mania—delusions or hallucinations that feel completely real. These might be mood-congruent (like believing you have special powers) or mood-incongruent (paranoid delusions unrelated to your elevated mood).
The depressive episodes in bipolar I can be severe and prolonged, but people with this subtype actually spend less time depressed than those with bipolar II. The manic episodes tend to be more dramatic and easier to identify, which paradoxically leads to faster diagnosis.
Bipolar II Disorder Symptoms
Bipolar II requires at least one hypomanic episode and one major depressive episode, with no history of full mania. The hypomanic episodes are shorter (four days minimum) and less impairing than mania, but the depressive episodes are just as severe as in bipolar I.
People with bipolar II spend significantly more time depressed than those with bipolar I. The depressive episodes tend to be longer, more frequent, and more treatment-resistant. Suicide risk in bipolar II equals or exceeds that of bipolar I, largely because of the chronic depressive burden.
The hypomania in bipolar II often goes unrecognized because it feels good and doesn’t cause obvious impairment. You might have four-day periods of high productivity, creativity, and confidence that you attribute to “finally feeling like myself” rather than recognizing them as mood episodes.
That’s why understanding the difference between bipolar I and II matters for treatment. Bipolar II isn’t “bipolar lite”—it’s a distinct condition with its own challenges and treatment needs.
Cyclothymic Disorder Symptoms
Cyclothymic disorder involves chronic fluctuation between hypomanic symptoms and depressive symptoms for at least two years (one year in children and adolescents). The symptoms never meet full criteria for hypomanic or major depressive episodes, but they’re present more days than not.
You might have a few good weeks where you’re energized and productive, followed by a few weeks of low mood and fatigue, then back up again. The cycles are unpredictable and exhausting. You never feel stable.
Cyclothymic disorder often develops in adolescence or early adulthood. About 15-50% of people with cyclothymia eventually develop bipolar I or II disorder, which is why early identification and monitoring matter.
The challenge with cyclothymia is that the symptoms are chronic but subsyndromal—not quite severe enough to meet episode criteria, but definitely impairing your functioning and quality of life. Treatment focuses on mood stabilization and preventing progression to full bipolar disorder.
Between Episodes: Residual and Subsyndromal Symptoms
The myth of bipolar disorder is that you’re either in an episode or you’re fine. The reality is that most people experience residual symptoms between episodes—lingering depression, mild anxiety, sleep disturbances, or cognitive difficulties that never fully resolve.
Subsyndromal symptoms are symptoms that don’t meet full episode criteria but are still present and impairing. You might have three depressive symptoms instead of five, or two days of elevated mood instead of four. These symptoms predict the next full episode and represent opportunities for early intervention.
Research on recovery outcomes shows that only 35% of people with bipolar I mania achieve sustained clinical recovery over 28 weeks, even with treatment. The rest continue experiencing symptoms that interfere with work, relationships, and daily functioning.
Common residual symptoms include:
- Mild depressive symptoms (low energy, anhedonia, poor concentration)
- Sleep disturbances (difficulty falling asleep, early waking, irregular sleep schedule)
- Anxiety symptoms (worry, restlessness, physical tension)
- Cognitive difficulties (memory problems, slow processing speed, executive dysfunction)
- Irritability or mood lability
Your true baseline is what you experience between episodes when you’re most stable. Identifying that baseline helps you recognize when symptoms are emerging and when to adjust your management protocol.
Tracking Your Symptoms
A mood tracking inventory is your most powerful tool for understanding your polarity pattern and identifying your earliest warning sign. You’re looking for patterns that predict episodes before they fully develop.
Track at least three data points daily: mood (on a scale from depressed to elevated), sleep (hours and quality), and energy level. Add any symptoms you notice—racing thoughts, irritability, loss of interest, changes in appetite, risky behavior, suicidal thoughts.
Essential tracking elements:
- Mood rating (-3 to +3 scale: -3 = severely depressed, 0 = baseline, +3 = manic)
- Sleep (hours, quality, whether you felt rested)
- Energy level (low, normal, elevated)
- Specific symptoms (racing thoughts, irritability, anhedonia, etc.)
- Triggers (stressors, schedule changes, medication changes, substance use)
- Menstrual cycle (if applicable—hormones affect mood cycling)
Use a simple app, spreadsheet, or paper chart—whatever you’ll actually use consistently. The goal isn’t perfection. It’s creating a record that reveals your trigger-and-response patterns over time.
After a few months, you’ll start seeing patterns. Maybe your sleep gets disrupted three days before hypomania emerges. Maybe irritability is your earliest warning sign of depression. Maybe seasonal changes or work stress consistently trigger episodes.
That pattern recognition allows you to intervene early—adjusting sleep, contacting your psychiatrist, increasing therapy sessions, or implementing your crisis plan before you’re in full episode. For more tools and strategies, explore our bipolar disorder tools section.
When to Seek Help
Seek immediate help if you’re experiencing suicidal thoughts, psychotic symptoms, or engaging in dangerous behavior. Call 988 (Suicide and Crisis Lifeline) or go to your nearest emergency room. Mixed features with agitation and hopelessness require urgent evaluation.
Schedule an appointment with a psychiatrist if you’re experiencing:
- Mood episodes lasting more than a few days that interfere with work or relationships
- Sleep disturbances that persist despite good sleep hygiene
- Significant changes in energy, activity level, or behavior
- Risky or impulsive behavior that’s out of character
- Depressive symptoms that don’t respond to treatment or worsen on antidepressants
Bring your mood tracking data to the appointment. A clear history of mood patterns helps clinicians distinguish between bipolar disorder, major depression, and other conditions. If you’ve had periods of elevated mood—even if they felt good—mention them specifically.
If you’re already diagnosed with bipolar disorder but experiencing breakthrough symptoms, contact your treatment team. Don’t wait until you’re in crisis. Early intervention prevents full episodes and reduces the cumulative burden of mood cycling.
Consider connecting with bipolar support groups where you can learn from others’ experiences with symptom recognition and management. Peer support complements professional treatment and helps you feel less alone in navigating this condition.
Charting Your Next Baseline
Understanding bipolar disorder symptoms isn’t about memorizing a list. It’s about learning to read your own nervous system, recognizing your polarity pattern, and building cycle awareness that guides every treatment decision you make.
Your earliest warning sign is different from everyone else’s. For some people, it’s disrupted sleep. For others, it’s irritability, racing thoughts, or loss of interest in daily activities. Identifying that signal gives you a window for intervention before you’re deep in an episode.
The symptoms you experience depend on your subtype, but the management principles remain consistent: protect your sleep architecture, track your mood patterns, match the intervention to your episode, and maintain nervous system regulation through consistent routines.
Start your mood tracking inventory today—even if you’re stable right now. The data you collect during baseline periods becomes invaluable when symptoms emerge. You’ll have a reference point for what “normal” looks like for you, making it easier to spot deviations early.
Work with your treatment team to develop a personalized management protocol that addresses your specific symptom pattern. That might include medication options, talk therapy, lifestyle changes, or a combination of approaches.
Remember: sustainable stability comes from understanding your unique presentation, not from trying to fit into a textbook description. Your symptoms, your triggers, and your response to treatment are all part of your individual polarity pattern. Learning to read that pattern is how you move from reactive crisis management to proactive mood stabilization.
Frequently Asked Questions
What’s the difference between mania and hypomania? Mania lasts at least seven days and causes marked impairment in functioning, often requiring hospitalization and sometimes including psychotic features. Hypomania lasts at least four days with similar symptoms but less intensity, no significant impairment, no hospitalization, and no psychosis. The distinction determines whether you have bipolar I or II.
Can you have bipolar disorder without manic episodes? Yes—that’s bipolar II disorder. You experience hypomanic episodes (shorter, less severe) and major depressive episodes but never full mania. Bipolar II isn’t milder than bipolar I; people with bipolar II actually spend more time depressed and have comparable suicide risk.
Why do antidepressants sometimes make bipolar disorder worse? Antidepressants without mood stabilizers can trigger mania, hypomania, or rapid cycling in up to 25% of people with bipolar disorder. They work by increasing neurotransmitter activity, which can destabilize mood regulation when your brain’s circuitry is already prone to cycling. That’s why the right med for the wrong cycle can cause more harm than no medication.
How long do bipolar episodes typically last? Manic episodes average 3-6 months untreated, hypomanic episodes last at least 4 days, and depressive episodes typically last 6-12 months without treatment. With proper treatment, episodes shorten significantly. Individual patterns vary widely—some people have rapid cycling (four or more episodes per year), while others have years between episodes.
What are mixed features and why are they dangerous? Mixed features occur when you experience symptoms from both poles simultaneously—like feeling depressed and hopeless while also having racing thoughts and agitation. They’re dangerous because they combine the suicidal ideation of depression with the energy and impulsivity of mania, creating the highest suicide risk of any bipolar presentation.
How do I know if I’m experiencing symptoms or just normal mood changes? Bipolar symptoms are more intense, last longer, and cause functional impairment compared to normal mood fluctuations. If mood changes interfere with work, relationships, or daily activities for more than a few days, or if you notice decreased sleep need, racing thoughts, or significant behavior changes, track the symptoms and consult a mental health professional.