
What to Expect in a Psychiatric Emergency Room: A Guide for People With Bipolar Disorder
You do not go to a psychiatric ER because you want drama. You go because something feels dangerous, or because someone who loves you can see that the ground is giving way under your feet.
If you live with bipolar disorder, you may already know how easy it is to doubt yourself in the worst moment. You may fear being dismissed, locked in, judged, or left waiting for hours while your mind is on fire.
This guide is here to lower some of that fear. It is for preparation and education, not for talking you out of getting urgent help.
If You Are In Crisis Right Now
If you need the emergency room, stop reading and go. If your safety is at risk, this is not the moment to gather more information.
Call 911 if you cannot get there safely on your own. Call or text 988 if you are not sure whether you need emergency care, because a crisis counselor can help you assess the situation.
This guide is not a reason to wait when waiting is dangerous. If your gut, your support person, your prescriber, or a 988 counselor says this has crossed into emergency territory, listen.
When Going To The Psychiatric ER Is The Right Decision
Bipolar disorder can push the brain into states where judgment, impulse control, and reality testing start to break down. That is the plain-English reason the ER matters, because sometimes the part of you that usually keeps you safe is not fully online.
The clinical words may be mania, psychosis, severe depression, or suicidal crisis. But before the jargon, the real question is simpler: can you stay alive and safe without immediate, in-person help?
Situations That Warrant Immediate ER Care
Go to the ER right away if you have a specific suicide plan and access to the means to carry it out. Go right away if you have already overdosed, hurt yourself, or taken any action that could seriously injure or kill you.
Go if you are hearing or seeing things that are not there, or if you are deeply convinced of something that shows you have lost contact with reality. Go if mania has become dangerous and you cannot stop the behavior, especially if you are not sleeping, spending wildly, driving unsafely, becoming aggressive, or putting yourself at serious risk.
Go if you are so unwell that you cannot care for your basic needs. That can mean not eating for days, not managing hygiene, wandering, getting lost, or being unable to keep yourself safe.
Go if your support person believes your safety is at immediate risk and you cannot safely wait for an outpatient appointment. Go if your prescriber or a 988 counselor tells you to go.
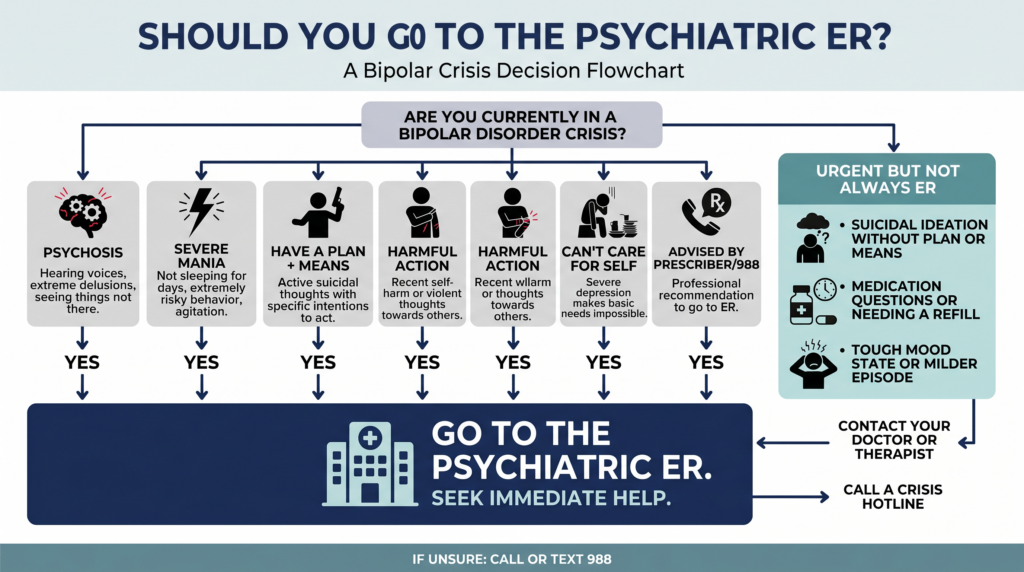
Situations That Do Not Always Require The ER
Not every bipolar crisis belongs in the ER. Some moments are urgent without being immediately life-threatening.
If you are having suicidal thoughts but do not have a specific plan or access to means, that still matters, and you should reach out the same day to your prescriber or 988. If you are in a rough mood state that feels bad but not imminently dangerous, contact your prescriber urgently and ask what to do next.
If your concern is mostly about medication side effects or questions, your prescriber is usually the better first call. The ER is best used for acute safety situations, not for ongoing crisis counseling or routine med management.
Preparing To Go To The ER
In bipolar disorder, stress can strip your thinking down to survival mode. That means details get foggy, timelines blur, and simple questions can suddenly feel impossible to answer.
A little preparation can help the staff help you faster. It can also reduce the chance that you minimize what is happening because you are scared, ashamed, or exhausted.
What To Bring
Bring a list of your current medications, doses, and prescribers if you can. If that is too hard, bring the bottles themselves.
Bring your insurance card and photo ID. Bring your psychiatrist’s name and contact information, plus the name and phone number of your main support person.
If you have a psychiatric advance directive, bring it or keep it accessible on your phone. If you think you may be there for a long time, bring comfortable clothing and a phone charger.
What To Tell ER Staff
Say it plainly: “I have bipolar disorder and I am in a psychiatric emergency.” That one sentence helps staff understand the frame right away.
Then be specific about why you are there. “I have been having thoughts of suicide with a specific plan” tells them much more than “I’m not feeling well.”
If you are there with a loved one, give concrete facts. Say, “He has not slept in three days and thinks strangers are sending him messages,” not “He’s acting weird.”
Do not downplay your symptoms in the ER. This is one place where being blunt protects you.
What Happens In A Psychiatric ER: The Process
A psychiatric ER visit can feel disorienting because a lot happens out of order from your point of view. You may answer the same question several times, wait longer than you expected, and still not know what the plan is for a while.
That does not always mean something is wrong. It often means the system is trying to sort out safety, medical stability, and the least restrictive next step.
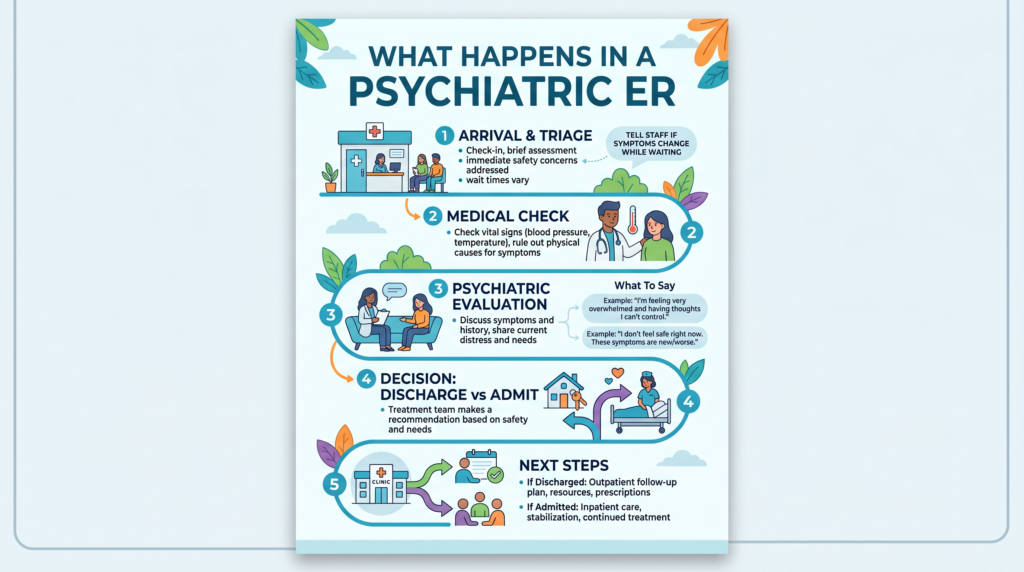
Arrival And Triage
Triage is the first sort. A nurse or intake staff member will assess how urgent your situation is and whether there is an immediate safety issue.
Psychiatric triage focuses heavily on danger to self, danger to others, psychosis, severe mania, severe depression, and ability to care for yourself. You may still have to wait, and that is common, especially if several people arrive in crisis at once.
If your symptoms get worse while you are waiting, tell staff right away. Do not assume they know that you have moved from scared to actively unsafe.
Medical Assessment
Sometimes the brain looks psychiatric when the body is actually driving the problem. That is why many ERs do some level of medical clearance before the psychiatric evaluation.
This may include vital signs, blood work, a urine drug screen, or a physical exam. The goal is to rule out medical causes, check for intoxication or overdose, and make sure you are physically stable enough for psychiatric care.
Psychiatric Evaluation
Once you are medically cleared, or medically stable enough, you will usually be seen by a psychiatrist, psychiatric resident, nurse practitioner, social worker, or another mental health clinician. They are trying to build a safety picture, not catch you in a mistake.
They will ask about your current symptoms, your bipolar history, your medications, any past hospitalizations, what happened today, whether you have support, and whether you can stay safe outside the hospital. Be as honest and concrete as you can, even if it feels embarrassing.
You can usually ask to have a support person present, though there are situations where the team may need to speak with you alone first. If you cannot explain clearly, your support person can often fill in missing details.
What The Clinician Is Deciding
The main decision is whether you can be safely managed in the community or whether you need inpatient care. That is the heart of the whole visit.
One 2023 study from Hannover Medical School found that about 54.5% of psychiatric emergency presentations led to inpatient admission. In plain terms, roughly half of people were admitted and roughly half were discharged with some kind of outpatient plan.
Things that make discharge more likely include a lower immediate safety risk, a workable safety plan, a reliable support person, and fast outpatient follow-up. Things that make admission more likely include psychosis, inability to care for yourself, no safe support system, serious suicidal risk, or symptoms so severe that medication changes need close observation.
Possible Outcomes
You may be discharged with a safety plan and follow-up instructions. Ideally, that includes a concrete next appointment, any medication changes, and clear guidance on what to do if things worsen.
You may be referred to a crisis stabilization unit, often called a CSU. This is a middle level of care, less restrictive than inpatient hospitalization but more structured than going straight home.
You may agree to voluntary psychiatric hospitalization. In that case, you are admitted because you and the team agree you need a safer, more contained setting.
You may also be placed on an involuntary psychiatric hold if you meet your state’s legal criteria for imminent danger to yourself or others and refuse care. The exact rules depend on where you live, but the basic idea is immediate safety overrules refusal in very specific situations.
How Long The Process Takes
A psychiatric ER visit often moves at the speed of a strained system, not at the speed of your fear. That mismatch can feel brutal.
You may think, “If this is serious, why am I waiting?” The answer is usually capacity, not disbelief.
Reality Of Wait Times
Waits of 4 to 12 hours are not unusual in many parts of the United States. The evaluation itself may take 1 to 3 hours, but waiting for the evaluation or for a bed can take much longer.
If you are waiting, try to use the time in simple ways. Rest if you can, sip water if allowed, and let your support person know where you are.
Boarding In Psychiatric ERs
“Boarding” means you have been evaluated and need inpatient care, but no psychiatric bed is available yet. So you remain in the ER and wait.
This can last many hours, and in some places it can last days. It is a documented crisis in psychiatric care, not a sign that your case has been forgotten.
If you are boarding, ask what is happening and what the current timeline looks like. You deserve updates, even if the update is “we are still waiting.”
Your Rights In The Psychiatric ER
A psychiatric emergency does not erase your personhood. Even when you are scared, confused, or too drained to argue, you still have rights.
The exact rules can change if you are on an involuntary hold or in an immediate safety emergency. But the baseline is that you are still a patient, not a problem.
What You Retain
You generally have the right to know what is being recommended and why. You generally have the right to consent to or refuse treatment, unless there is a legal or emergency exception.
You usually have the right to have a support person notified of where you are. You also usually have the right to make phone calls and to be treated with dignity.
If You Feel You Are Being Treated Dismissively
Say clearly, “I have bipolar disorder, I am in crisis, and I need a psychiatric evaluation.” Calm and specific often works better than trying to prove how bad things are through emotion alone.
If your concerns are not being addressed, ask for a patient advocate or social worker. If a support person is available, ask them to help advocate for you.
After The ER: If You Are Discharged
Discharge is not the end of the crisis. It is the handoff, and handoffs are fragile.
The brain and body are often wrung out after an ER visit. You may feel relief, shame, anger, confusion, or all of it at once.
Before You Leave
Make sure you know exactly what happens next. Do not settle for vague instructions if you are too foggy to fill in the blanks later.
Before you go, try to leave with a specific follow-up appointment, any new prescriptions or medication changes, clear return precautions, and crisis contact information. If anything is unclear, ask, “What should I do if I feel worse before my appointment?”
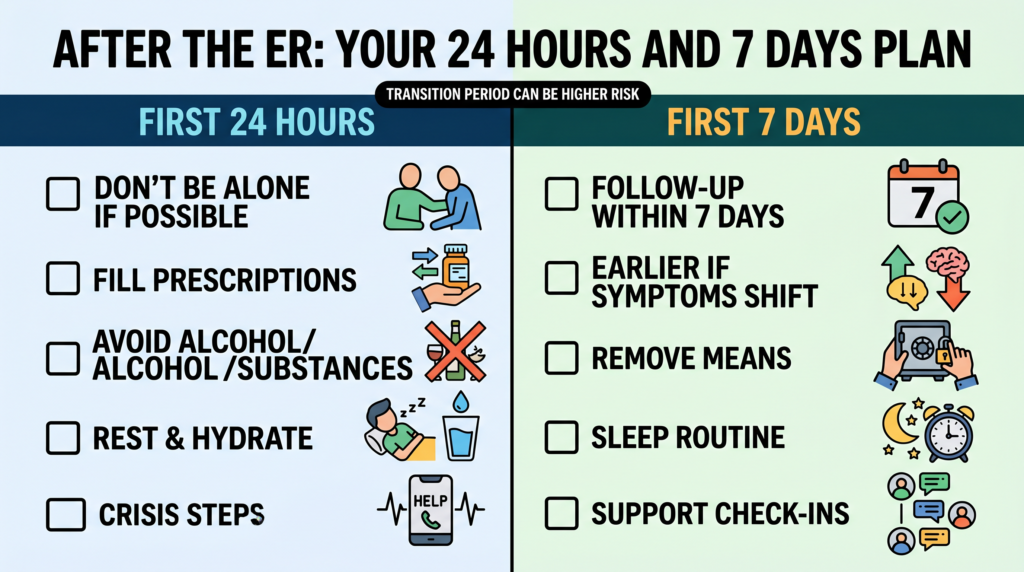
The First 24 Hours After Discharge
If possible, do not be alone. Ask your support person to stay with you or check in often.
Fill any new prescriptions right away. Avoid alcohol and substances, because they can make mood instability and impulsivity worse.
Use whatever post-crisis steps are in your safety plan. That might mean sleep protection, a quiet room, reducing stimulation, handing over car keys or credit cards for a day, or staying with someone safe.
Rest. Even if you did not get admitted, the visit itself is exhausting.
The First 7 Days After ER Discharge
The days right after psychiatric ER discharge are high-risk. Symptoms can swing back fast, and the stress of the visit can leave you feeling scraped raw.
Try to see your prescriber within 7 days, sooner if you can. If the ER did not set that up, call and ask for an urgent appointment, and reach out sooner if anything starts worsening.
Going To The ER With Someone You Love
Watching someone you love move into mania, psychosis, or suicidal crisis can feel like standing in a storm with no shelter. You may be trying to save them while also trying not to panic.
Your role matters. It can shape the accuracy of the evaluation more than you realize.
Your Role In The ER
You can give history your loved one may not be able to give clearly in the moment. With bipolar disorder, insight can drop sharply during mania, psychosis, or severe depression.
Be behavioral and factual. Say, “She has slept two hours total in three days, spent $4,000, and says the TV is sending her instructions,” rather than “She’s not herself.”
You may be asked to wait elsewhere during part of the evaluation. That is standard and does not necessarily mean you are being shut out.
What You Can And Cannot Do
You can provide information and advocate. You can ask to speak privately with the clinician to share safety concerns.
You cannot force treatment on a competent adult who refuses it, unless they meet legal criteria for involuntary evaluation or hospitalization. If you believe they do meet that threshold and the ER is missing it, ask to speak to the attending physician and state your concerns plainly and specifically.
Taking Care Of Yourself During The Wait
This kind of ER visit is hard on family and friends too. Your nervous system pays a price for it.
Bring water, a charger, and something to do if you can. Text someone you trust, breathe when you remember to, and let yourself admit that what you are witnessing is frightening.
After the visit, you may need your own debrief. That is not weakness. That is cleanup after a very human shock.
Charting Your Next Safe Step
A psychiatric ER visit is not a moral failure. It is not proof that you ruined your progress, and it is not evidence that you are too much for anyone to handle.
Sometimes it is just the place where danger gets named out loud. Sometimes it is the place where your brain, which has been dragging you toward an edge, finally meets a wall strong enough to hold.
If you think you may need the ER, trust the part of you that still wants to survive. If you are the one bringing someone you love, your calm, specific advocacy can help carry them through the worst hour until their mind comes back within reach.