IPSRT Bipolar Disorder: How It Works and What to Expect
You’ve tried the meds, you’ve tracked your moods, and you’ve read every article about sleep hygiene. But here’s what nobody tells you until you’re deep into managing bipolar disorder: the chaos isn’t just chemical.
It’s also about the thousand tiny disruptions to your daily rhythm that pile up until your nervous system can’t tell Tuesday from Saturday, 9am from midnight, or a normal social commitment from an episode trigger. IPSRT bipolar disorder treatment addresses exactly this gap, and it does so by treating your daily routine as seriously as your medication protocol.
Interpersonal and Social Rhythm Therapy isn’t just another talk therapy repackaged with a new acronym. It’s a specific, structured intervention built on decades of clinical data showing that people with bipolar disorder are exquisitely sensitive to disruptions in daily routines, and that stabilizing those rhythms can prevent episodes as effectively as adding another medication to your regimen.
You’ll learn to track not just your mood but the scaffolding that holds your mood steady: when you wake, when you eat, when you see other people, and how regular those patterns stay week to week.
Key Takeaways
- IPSRT combines two evidence-based approaches: interpersonal therapy to resolve relationship stress and social rhythm therapy to stabilize daily routines, both of which directly impact mood stability in bipolar disorder
- Your daily routine acts as a biological anchor: irregular sleep, meals, and social contact can trigger episodes by disrupting circadian rhythms, which are already vulnerable in bipolar disorder
- The Social Rhythm Metric is your primary tool: you’ll track 17 daily activities and rate their regularity, giving you and your therapist concrete data about which disruptions precede mood shifts
- IPSRT works in three phases: initial assessment and history-taking, acute treatment targeting current symptoms and rhythm disruptions, and maintenance focused on preventing future episodes
- Realistic outcomes take time: most people see meaningful rhythm stabilization within 12-20 weeks, with the biggest gains in preventing depressive episodes and reducing rapid cycling
What Is IPSRT?
IPSRT stands for Interpersonal and Social Rhythm Therapy, a manualized psychotherapy developed specifically for bipolar disorder by Dr. Ellen Frank and colleagues at the University of Pittsburgh in the 1990s.
It operates on a straightforward premise: bipolar disorder makes your internal clock hypersensitive to disruption, and interpersonal stress is one of the most reliable disruptors of daily routines. Fix both problems simultaneously, and you create a buffer against the next episode.
The therapy pulls from two established traditions. The interpersonal component comes from Interpersonal Psychotherapy (IPT), originally designed for depression, which focuses on four problem areas: grief, role disputes, role transitions, and interpersonal deficits.
The social rhythm component is unique to IPSRT and centers on stabilizing the timing of daily activities that serve as zeitgebers—external cues that entrain your circadian system.
You won’t spend sessions diving into childhood trauma or deconstructing cognitive distortions. Instead, you’ll work on concrete problems: the coworker conflict that’s keeping you up at night, the grief over a relationship that ended during your last manic episode, or the fact that your weekend sleep schedule differs from your weekday schedule by four hours.
Managing Bipolar Disorder Symptoms Through Interpersonal and Social Rhythm therapy recognizes that these aren’t minor lifestyle issues—they’re direct threats to your stability.
The Scientific Foundation: Why Social Rhythms Matter
The Circadian-Bipolar Connection
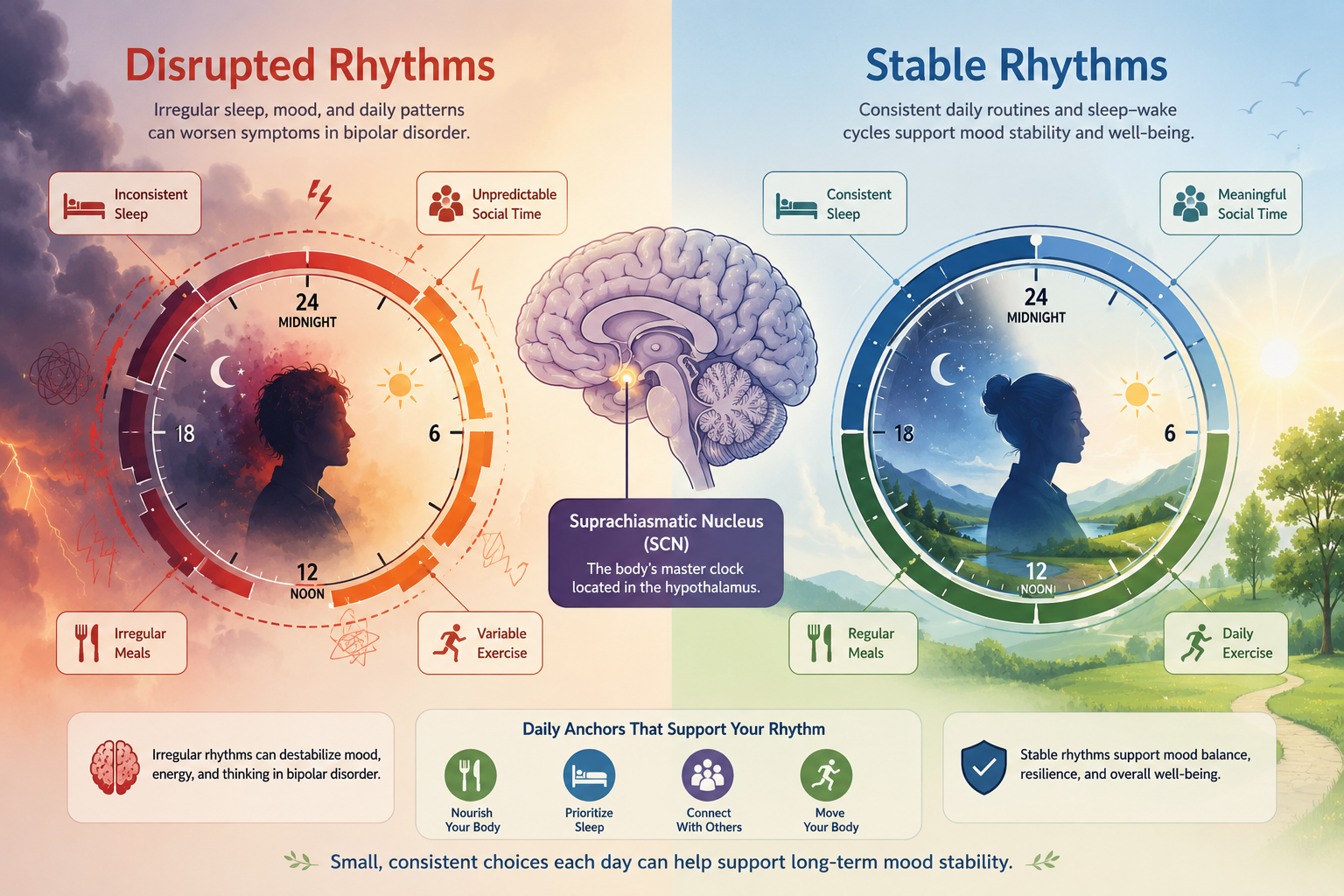
Your brain’s master clock sits in the suprachiasmatic nucleus, a tiny cluster of neurons that coordinates everything from hormone release to body temperature to the sleep-wake cycle. In bipolar disorder, this system appears to be both more fragile and more powerful than in neurotypical brains. Small disruptions—a single night of poor sleep, a skipped meal, an unexpected social obligation—can cascade into larger rhythm disturbances that destabilize mood.
When your circadian rhythms get knocked off schedule, your brain’s reward circuitry and stress response systems lose their normal daily pattern. Cortisol spikes at the wrong times, melatonin release gets delayed or blunted, and the neurochemical environment that keeps mood stable starts to drift. For someone without bipolar disorder, this might mean feeling groggy or irritable for a day.
For you, it can be your earliest warning sign that a depressive or manic episode is building.
The mechanism works both ways. Mood episodes disrupt routines (you can’t maintain a regular sleep schedule during mania, and you can’t keep social commitments during depression), and disrupted routines trigger mood episodes. IPSRT aims to break this cycle by making rhythm stability a treatment target as concrete as medication adherence.
The Research Evidence
The original IPSRT trials followed patients with bipolar I disorder for up to two years, comparing those who received IPSRT plus medication to those who received intensive clinical management plus medication. The IPSRT group showed longer time to recurrence of any mood episode, particularly depressive episodes, and greater regularity in daily routines predicted better outcomes.
Effect sizes weren’t enormous—this isn’t a miracle cure—but they were clinically meaningful, especially for people who’d already tried multiple medication combinations without achieving sustainable stability.
More recent studies have extended these findings to bipolar II disorder and shown that IPSRT reduces rapid cycling when added to standard pharmacotherapy. The therapy appears most effective for preventing depression rather than mania, likely because depressive episodes are more strongly linked to rhythm disruptions like social withdrawal and irregular sleep.
If you’re someone whose pattern involves long depressive episodes with brief hypomanic periods, IPSRT may offer more protection than if your pattern is predominantly manic.
The data also shows that rhythm regularity itself—independent of therapy—predicts better outcomes. People who naturally maintain consistent daily schedules have fewer episodes and less severe symptoms. This suggests the intervention works through its proposed mechanism: by stabilizing the external cues that regulate your internal clock, you create a more stable neurochemical environment.
The Two Components of IPSRT
The interpersonal piece addresses the reality that relationship stress and mood episodes feed each other relentlessly. Your last manic episode may have damaged a friendship, your depression makes it hard to show up for your partner, or a major life transition has left you without the social support you need. These aren’t separate problems from your bipolar disorder—they’re part of the same system.
IPSRT uses a structured approach to interpersonal problems, organizing them into four categories. You and your therapist will identify which category best fits your current situation, then work systematically to resolve it. The goal isn’t to fix every relationship issue you’ve ever had but to address the one or two problems most directly connected to your mood instability right now.
Grief
Grief in IPSRT means mourning any significant loss: a death, a divorce, a job you loved, or even the loss of your pre-diagnosis identity. Unresolved grief disrupts routines (you stop going to places that remind you of the loss) and creates sustained low mood that can tip into a depressive episode. The therapy helps you process the loss while rebuilding the daily structure that grief dismantled.
Role Disputes
Role disputes happen when you and another person have incompatible expectations about your relationship. Your partner expects you to manage household tasks the way you did before your last depressive episode. Your boss expects consistent performance despite your need for flexible hours. These ongoing conflicts create chronic stress that destabilizes both your mood and your daily routine.
Role Transitions
Any major life change—starting a new job, becoming a parent, moving to a new city, retiring—counts as a role transition. Transitions disrupt established routines by definition, and they often involve loss of the old role alongside the challenge of the new one. Does Psychotherapy Help to Treat Bipolar Disorder? research shows that people with bipolar disorder are particularly vulnerable during transitions because the rhythm disruption happens exactly when stress is highest.
Interpersonal Deficits
This category covers social isolation and difficulty forming or maintaining relationships. If you don’t have enough meaningful social contact, you lose important zeitgebers (regular social activities that anchor your schedule) and the mood-protective effects of connection. The therapy focuses on building specific skills and creating opportunities for regular social interaction.
Component 2: Social Rhythm Therapy
Social rhythm therapy is where IPSRT diverges completely from standard talk therapy. You’ll use a specific tracking tool called the Social Rhythm Metric to monitor 17 daily activities: when you get out of bed, when you have your first contact with another person, when you start work or school, when you eat meals, when you exercise, when you return home, and when you go to bed. For each activity, you’ll note the time and rate how stimulating the social interaction was.
The Social Rhythm Metric (SRM)
The SRM isn’t a mood tracking inventory, though you’ll track mood alongside it. It’s a rhythm tracking inventory. You’re looking for patterns in the regularity of your daily activities, not just whether you felt good or bad. A high-regularity day means your activities happened at roughly the same time as the previous day. A low-regularity day means significant variation.
You’ll calculate a weekly average regularity score, and this number becomes a concrete target. If your baseline regularity is 3 out of 5, your goal might be to reach and maintain 4 out of 5. This isn’t about perfection—it’s about reducing the magnitude and frequency of disruptions. Weekend sleep-ins that push your wake time three hours later count as major disruptions. Skipping lunch because of a work deadline counts. Staying out until 2am at a concert counts.
From Tracking to Stability
The tracking phase typically lasts 2-4 weeks and serves two purposes. First, it gives you and your therapist data about which rhythm disruptions correlate with mood changes. You might discover that irregular meal times precede depressive symptoms by 48 hours, or that late bedtimes cluster in the week before hypomanic episodes. Second, it makes you aware of disruptions you weren’t consciously noticing.
Once you’ve established your baseline, you’ll work on protecting your sleep architecture and other key rhythms. This means saying no to social invitations that would push your bedtime too late, negotiating work schedules that allow consistent wake times, and planning ahead for unavoidable disruptions like travel or holiday gatherings. You’re building a management protocol based on your specific trigger-and-response patterns, not following generic sleep hygiene advice.

What IPSRT Sessions Look Like
Phase 1: Assessment and History
The first 3-5 sessions focus on building your interpersonal inventory and establishing your rhythm baseline. Your therapist will ask detailed questions about your relationships, your daily schedule, and the timeline of your mood episodes. You’re looking for connections:
Did your last depressive episode start after a conflict with your sister?
Did your most recent hypomanic period coincide with a week of irregular sleep due to a work project?
You’ll also complete the Social Rhythm Metric for the first time and discuss which activities are most important to stabilize. For most people, sleep and wake times are the highest priority, followed by meal times and social contact. Your therapist will help you identify your earliest warning signs of mood shifts and link them to specific rhythm disruptions.
This phase also includes psychoeducation about the circadian-bipolar connection. You need to understand the mechanism—why a disrupted Tuesday night affects your Thursday mood—to stay motivated when protecting your routine feels inconvenient or socially awkward.
Phase 2: Acute Treatment
Acute treatment typically runs 12-20 weekly sessions and targets both your current interpersonal problem and your rhythm irregularities. If you’re working on a role dispute with your partner, sessions will include communication skills practice and negotiation strategies. If you’re addressing grief, you’ll work through the stages of mourning while simultaneously rebuilding the routines that grief disrupted.
Throughout this phase, you’ll continue tracking your social rhythms and reviewing the data each session. Your therapist will help you spot patterns you might miss: the subtle rhythm disruption that happened three days before your mood dipped, or the week of high regularity that preceded your most stable period.
You’ll experiment with interventions—setting a consistent wake time even on weekends, scheduling regular social contact, protecting your evening routine—and track their effects.
The goal is to achieve both interpersonal resolution and rhythm stability. You want the role dispute resolved or at least managed, and you want your regularity score consistently in the target range. Talk Therapy for Bipolar: Full Guide to Types & Benefits shows that combined approaches like IPSRT tend to work better than single-focus interventions because they address multiple vulnerability factors simultaneously.
Phase 3: Preventive Maintenance
Once you’ve achieved stability, sessions typically shift to monthly or as-needed maintenance. The focus moves to preventing future episodes by maintaining rhythm regularity and catching early warning signs before they escalate. You’ll continue using the Social Rhythm Metric, though often in a simplified form, and you’ll have a written plan for managing predictable disruptions like travel, illness, or seasonal changes.
Maintenance also involves preparing for future interpersonal challenges. If you’ve resolved a role dispute, how will you handle the next conflict that arises? If you’ve worked through grief, how will you protect your stability if you experience another loss? You’re building a sustainable stability protocol that extends beyond the therapy relationship.
The Four Interpersonal Problem Areas in Practice
Identifying Your Problem Area
Most people entering IPSRT have multiple interpersonal issues, but the therapy asks you to focus on the one most directly connected to your current mood instability. Your therapist will help you choose by asking things like:
- Which problem is causing the most distress right now?
- Which one is most clearly disrupting your daily routine?
- Which one, if resolved, would have the biggest impact on your stability?
You might have unresolved grief about a relationship that ended during a manic episode, but if the immediate crisis is a role dispute with your boss that’s causing daily stress and irregular work hours, you’ll likely start there. The other issues don’t disappear—they just aren’t the primary focus of this treatment phase.
Working Through Grief in IPSRT
Grief work in IPSRT differs from traditional grief therapy because it explicitly connects the emotional process to routine disruption. You’re not just processing the loss—you’re also rebuilding the daily structure that the loss destroyed. If you lost a partner who was part of your evening routine, you need both to mourn that relationship and to establish new evening activities that provide structure and social contact.
The therapy uses specific techniques: reviewing the relationship and the circumstances of the loss, expressing the full range of emotions (including anger and relief, not just sadness), and gradually re-engaging with activities and people you’ve been avoiding. Throughout, you’re tracking how grief-related behaviors (social withdrawal, irregular sleep, skipped meals) affect your mood and working to maintain rhythm regularity even while grieving.
Working Through Role Disputes
Role disputes require clear communication about expectations and negotiation toward a mutually acceptable resolution. Your therapist will help you identify the specific disagreement (not the vague sense that “things aren’t working”), understand both your perspective and the other person’s, and decide whether the relationship can be renegotiated or needs to end.
The connection to social rhythms is direct: ongoing disputes create unpredictable stress that disrupts your routine. If you’re fighting with your roommate about household responsibilities, you might avoid being home, which disrupts your meal and sleep schedule.
If you’re in conflict with a family member, you might skip family gatherings that previously provided regular social contact. Resolving the dispute removes a major source of rhythm disruption.

Component 1: Interpersonal Therapy
Working Through Role Transitions
Role transitions involve mourning the old role, accepting the new one, and building routines appropriate to your new circumstances. If you’ve just become a parent, you need to grieve your pre-parent freedom and flexibility while establishing new daily rhythms that accommodate infant care. If you’ve lost a job, you need to mourn that identity while creating structure for your newly unstructured days.
The therapy helps you identify what you’ve lost, what you’ve gained, and what new skills or support you need. It also emphasizes maintaining as much rhythm regularity as possible during the transition. Even if your schedule has to change dramatically, you can keep some anchors consistent: the same wake time, the same morning routine, regular contact with specific people.
What Makes IPSRT Different From General Therapy
Standard psychotherapy for bipolar disorder often focuses on medication adherence, recognizing warning signs, and managing symptoms once they appear. IPSRT does all of that but adds a preventive layer by treating your daily routine as a therapeutic intervention in itself. Your sleep schedule isn’t just a lifestyle factor—it’s part of your treatment protocol, as important as taking your medication at the right time.
The therapy is also more structured and directive than many approaches. You’ll have homework every week: tracking your social rhythms, trying specific communication strategies, scheduling particular activities. Your therapist will review concrete data (your SRM scores, your mood ratings) rather than relying solely on your subjective report of how the week went. This structure works well for people who find open-ended therapy frustrating or who need clear targets to work toward.
IPSRT also differs in its explicit focus on cycle awareness before treatment selection. You need to understand your polarity pattern—whether you cycle more toward depression or mania, how long your episodes typically last, what your earliest warning signs are—before you can effectively use the therapy. Bipolar Disorder Symptoms vary so much between individuals that a one-size-fits-all approach rarely works.
Finally, IPSRT acknowledges the side-effect trade-off inherent in bipolar treatment. What are the Common Side Effects of Bipolar Disorder Medications? can include weight gain, sedation, and cognitive dulling, all of which affect your ability to maintain regular routines. The therapy helps you work with your prescriber to find the right med for the wrong cycle—medications that control symptoms without making rhythm regularity impossible.
Finding an IPSRT Therapist
IPSRT requires specific training beyond general psychotherapy credentials. Your therapist needs to understand the manualized protocol, know how to use the Social Rhythm Metric, and have experience working with bipolar disorder. Not every therapist who treats bipolar disorder has IPSRT training, and not every therapist who’s heard of IPSRT has completed formal certification.
Start by asking potential therapists directly: “Have you completed training in IPSRT? How many patients with bipolar disorder have you treated using this approach?” You want someone who can answer with specifics, not someone who’s read about it and thinks they can improvise. The International Society for Interpersonal Psychotherapy maintains a therapist directory that includes IPSRT-trained clinicians, though coverage varies by region.
If you can’t find an IPSRT-trained therapist locally, consider telehealth options. Many IPSRT specialists offer remote sessions, and the therapy translates well to video format since much of the work involves reviewing tracking data and practicing communication skills. Bipolar Disorder Treatment increasingly includes remote options, especially for specialized interventions like IPSRT.
You’ll also want to confirm that your therapist can coordinate with your psychiatrist or prescriber. IPSRT works best as part of a comprehensive treatment plan that includes medication, and your therapist needs to communicate with your medical team about rhythm disruptions that might signal the need for medication adjustments.
What to Expect: Realistic Outcomes
IPSRT won’t cure your bipolar disorder, and it won’t eliminate all episodes. What it can do is reduce the frequency and severity of episodes, particularly depressive ones, and give you more control over your stability.
Most people who complete a full course of IPSRT report feeling less at the mercy of their disorder—they can see episodes coming earlier, they know which disruptions to avoid, and they have concrete tools for getting back on track when life inevitably knocks them off schedule.
The timeline for seeing benefits typically runs 12-20 weeks for initial rhythm stabilization and interpersonal progress, with continued gains over 6-12 months as you practice maintaining regularity through various challenges. Some people notice changes quickly—within a few weeks of stabilizing their sleep schedule, their mood becomes noticeably more stable. Others need several months to see clear patterns in their tracking data and learn which interventions work for them.
The therapy demands consistent effort. You’ll track your rhythms every day, attend weekly sessions, complete homework assignments, and make sometimes uncomfortable changes to your social life and daily habits. If you’re in a phase where you can’t commit to that level of engagement, it’s worth waiting until you can rather than starting and stopping repeatedly.
IPSRT also requires accepting that protecting your stability sometimes means disappointing other people. You’ll turn down invitations that would disrupt your sleep schedule. You’ll set boundaries with family members whose demands create stress.
You’ll prioritize your routine over spontaneity. For some people, this feels like a reasonable trade-off. For others, it feels like letting the disorder win. Your therapist will help you find a balance that maintains both stability and quality of life, but there’s no denying that nervous system regulation requires some sacrifice.
Long-term, the goal is for rhythm maintenance to become automatic rather than effortful. You’ll internalize the awareness of which disruptions matter and develop habits that protect your key rhythms without constant conscious attention. You’ll still need to track periodically and stay alert to your earliest warning signs, but the daily work becomes less burdensome as the patterns become ingrained.
The research shows that people who achieve good rhythm regularity during acute treatment and maintain it afterward have significantly better outcomes than those who don’t. Your true baseline—the level of stability you can sustain long-term—depends partly on your medication regimen, partly on your life circumstances, but also significantly on how consistently you maintain regular daily rhythms. IPSRT gives you the tools to find and protect that baseline.
Frequently Asked Questions
How is IPSRT different from CBT for bipolar disorder?
Cognitive Behavioral Therapy focuses on identifying and changing thought patterns that contribute to mood episodes, while IPSRT focuses on stabilizing daily routines and resolving interpersonal problems. CBT asks “What are you thinking?” while IPSRT asks “What time did you wake up, and who did you interact with?” Both can be effective, and some people benefit from combining elements of each approach.
Can I do IPSRT if I’m currently in an episode?
IPSRT works best when you’re relatively stable, though “relatively” is the key word. If you’re in a severe manic or depressive episode, you’ll likely need to stabilize with medication first. But if you’re experiencing mild to moderate symptoms, you can start IPSRT and use it to prevent the episode from worsening. Your therapist will adjust the pace based on your current state.
Do I have to track my rhythms forever?
Most people track intensively during acute treatment, then shift to periodic tracking (a few days each month) during maintenance. Some people find that tracking becomes so automatic they don’t need the formal tool anymore. Others prefer to continue tracking because it helps them catch warning signs early. There’s no single right answer—it depends on what works for your management protocol.
Will IPSRT help with rapid cycling?
Research suggests IPSRT can reduce rapid cycling by stabilizing the rhythm disruptions that often trigger quick mood shifts. However, rapid cycling is complex and usually requires careful medication management alongside therapy. IPSRT alone won’t solve rapid cycling, but it can be a valuable part of a comprehensive treatment approach.
What if my work schedule makes regular rhythms impossible?
Shift work, irregular hours, and frequent travel do make IPSRT more challenging, but not impossible. The therapy helps you identify which rhythms you can control (meal times, social contact, morning routine) even when work hours vary. You’ll also work on strategies for minimizing the impact of unavoidable disruptions and recovering quickly when they occur.
How do I know if IPSRT is working?
You’ll see progress in your Social Rhythm Metric scores (higher regularity), longer periods between mood episodes, less severe symptoms when episodes do occur, and better ability to catch and respond to early warning signs. Your therapist will help you track these outcomes systematically rather than relying on subjective impressions.
Charting Your Next Baseline
You’ve spent years learning that bipolar disorder requires lifelong management, that there’s no quick fix, that stability means constant vigilance. IPSRT doesn’t change those realities, but it does offer something concrete to be vigilant about. Instead of waiting anxiously for the next episode to announce itself, you can track the rhythm disruptions that precede it.
Instead of feeling helpless when stress builds, you can address the specific interpersonal problem that’s destabilizing you.
The therapy asks you to take your daily routine as seriously as your medication, to see the connection between Tuesday’s skipped lunch and Thursday’s mood dip, to understand that protecting your sleep architecture isn’t optional self-care but essential treatment. It gives you a framework for understanding why some weeks feel stable and others feel precarious, and it provides tools for tipping the balance toward stability more often.
Start by tracking your current rhythms for a week, even before you find a therapist. Use a simple notebook or phone app to record when you wake, eat, interact with others, and sleep. Note which days feel regular and which feel chaotic. Look for patterns between rhythm disruption and mood changes. This baseline data will be valuable whether you pursue formal IPSRT or simply use the principles to inform your self-management.
If you decide to pursue IPSRT, approach it with realistic expectations and genuine commitment. The therapy works, but it works through consistent effort over months, not through sudden insight or dramatic breakthrough.
You’re building new habits and new awareness, and that process is gradual. Give yourself credit for small improvements: a week of consistent wake times, a difficult conversation handled well, a rhythm disruption caught and corrected before it triggered an episode.
Your stability matters, and the daily rhythms that support it matter. IPSRT simply makes that truth explicit and gives you a structured way to act on it. Whether you complete a full course of therapy or just incorporate some of the principles into your existing treatment plan, understanding the connection between your routines and your mood gives you more control over your trajectory.
That’s not a cure, but it’s something real and valuable: a way to work with your disorder rather than just enduring it.