Side Effects of Bipolar Disorder Medications: What to Expect and How to Manage Them
You’ve finally found a medication that’s working. The mania isn’t breaking through every few months, the depression isn’t pinning you to the bed for weeks at a time, and you’re starting to recognize what your true baseline actually feels like.
Then the tremor starts. Or the weight gain. Or the brain fog that makes you feel like you’re thinking through wet cotton.
Suddenly you’re facing a choice nobody prepared you for: the side-effect trade-off between mood stability and the physical toll these medications exact on your body.
Understanding bipolar disorder medication side effects isn’t about scaring you away from treatment—it’s about giving you the plain English information you need to make informed decisions, recognize warning signs early, and work with your prescriber to find sustainable stability.
The decades of clinical data show that most people with bipolar disorder need medication for long-term management, but the path to the right protocol often involves navigating side effects, adjusting doses, and sometimes switching medications entirely.
Key Takeaways
- Lithium remains the gold standard for bipolar I maintenance but requires consistent blood monitoring for kidney function, thyroid levels, and drug concentration to prevent toxicity
- Metabolic side effects from atypical antipsychotics (weight gain, diabetes risk, cholesterol changes) are the most clinically significant concern and require proactive monitoring starting at baseline
- The rash risk with lamotrigine is real but manageable through slow dose titration—serious reactions occur in only 0.1% of patients when titration protocols are followed correctly
- Side effects are the primary reason people stop taking bipolar medications, making it essential to match the intervention to your episode type and discuss tolerability concerns before they become deal-breakers
- Most side effects follow predictable patterns: some emerge immediately and fade within weeks, others develop gradually over months, and a few require immediate medical attention
Why Side Effects Matter So Much in Bipolar Treatment
Here’s what the research shows clearly: medication adherence determines outcomes in bipolar disorder more than almost any other factor. When you stay on an effective medication regimen, your risk of relapse drops by roughly 60% compared to stopping treatment.
But here’s the problem—up to 50% of people with bipolar disorder stop taking their medications within the first year, and side effects rank as the number one reason.
This creates a brutal paradox. The medications that stabilize your mood often come with physical effects that feel intolerable, making you want to stop the very treatment that’s keeping you stable. You’re not being difficult or non-compliant when you struggle with this—you’re responding rationally to real physical discomfort.
The key is cycle awareness before treatment selection. Before you and your prescriber choose a medication, you need to understand your polarity pattern—whether you cycle more toward mania, depression, or mixed states.
Someone whose bipolar disorder manifests primarily as depressive episodes will have different medication needs and side-effect tolerability than someone who experiences frequent manic episodes. Taking the right med for the wrong cycle can mean enduring side effects without getting the mood stabilization you actually need.
Your earliest warning sign of a side effect becoming a problem isn’t always the physical symptom itself—it’s the moment you start thinking about skipping doses. That’s your signal to contact your prescriber immediately, not to tough it out or make unilateral changes to your management protocol.

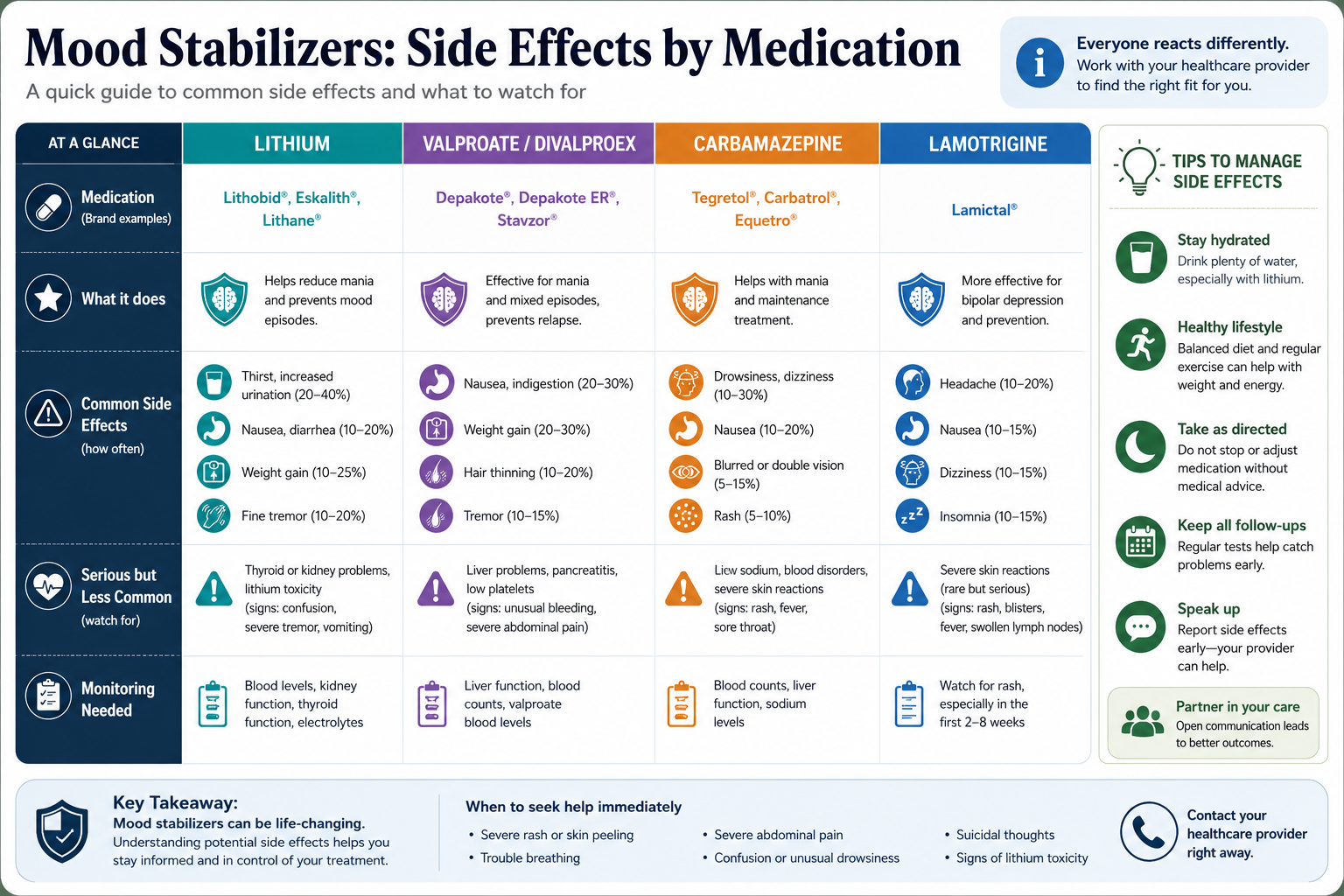
Mood Stabilizers: Side Effects by Medication
Lithium
Lithium works by modulating intracellular signaling pathways in your brain, essentially helping neurons communicate more predictably when your mood regulation system gets stuck in overdrive or shutdown mode. The clinical data spanning decades shows median relapse-free survival of 81 months for people taking lithium for bipolar I disorder—more than double the 36 months for valproate.
But lithium’s narrow therapeutic window means the difference between an effective dose and a toxic dose is smaller than with most psychiatric medications. This is why understanding the long-term side effects of lithium becomes essential for anyone considering this medication.
Common Early Side Effects
When you first start lithium, your body needs time to adjust to having this salt in your system at therapeutic levels. You’ll likely notice:
Gastrointestinal effects like nausea, diarrhea, or stomach discomfort hit about 30-40% of people in the first few weeks. Taking lithium with food usually helps, and these symptoms typically fade as your body adapts.
Hand tremor appears in roughly 25% of people on lithium. It’s usually a fine tremor—your hands shake slightly when you hold them out or try to do detailed work. The tremor often improves after the first month, but for some people it persists and requires either dose adjustment or adding a beta-blocker.
Increased thirst and urination happen because lithium affects how your kidneys concentrate urine. You might find yourself drinking significantly more water and using the bathroom more frequently. This isn’t dangerous by itself, but it’s your body’s way of managing lithium levels.
Cognitive effects like mental fog, difficulty concentrating, or feeling slightly slowed down concern people more than almost any other side effect. About 20-30% of people report some cognitive dulling on lithium. For some, this improves after a few months; for others, it’s the side effect that makes lithium untenable long-term.
Side Effects Requiring Medical Attention
Some lithium side effects signal that your dose needs adjustment or that you’re developing a complication requiring intervention:
Significant tremor that interferes with daily activities—you can’t write legibly, hold a coffee cup steady, or do fine motor tasks—needs evaluation. Your prescriber might lower your dose, check your lithium level, or add propranolol.
Excessive urination (polyuria) beyond the initial increase, especially if you’re urinating more than 3 liters daily, can indicate nephrogenic diabetes insipidus. This is a condition where your kidneys lose their ability to concentrate urine properly. It’s reversible if caught early but can become permanent if ignored.
Hypothyroidism symptoms like fatigue, weight gain, cold intolerance, or depression developing after months on lithium occur in 15-20% of people. Lithium interferes with thyroid hormone production, which is why you need regular thyroid function tests.
Significant weight gain of more than 10-15 pounds over several months happens to about 20% of people on lithium. The mechanism isn’t fully understood but likely involves changes in metabolism and increased thirst leading to consuming more caloric beverages.
Lithium Toxicity — Recognize and Act
Lithium toxicity is a medical emergency. Your therapeutic blood level typically ranges from 0.6 to 1.2 mEq/L, but toxicity can begin above 1.5 mEq/L. The problem is that dehydration, certain medications (especially NSAIDs and some blood pressure drugs), or kidney problems can push your level into the toxic range even if you haven’t changed your dose.
Early toxicity signs include severe nausea, vomiting, diarrhea, pronounced tremor, confusion, and slurred speech. Severe toxicity causes seizures, irregular heartbeat, and kidney failure. If you experience these symptoms, you need emergency medical care immediately—don’t wait to call your prescriber.
Long-Term Monitoring Requirements
Lithium requires more consistent medical monitoring than most psychiatric medications. You’ll need blood tests to check your lithium level initially every week or two until you’re stable, then every 3-6 months long-term. You also need kidney function tests (creatinine, BUN, eGFR) and thyroid function tests (TSH, free T4) every 6-12 months.
This monitoring isn’t optional—it’s how you catch problems before they become serious. Many people find that setting up a standing lab appointment every six months helps them stay on track with monitoring requirements.
Valproate (Depakote/Divalproex)
Valproate works by increasing GABA activity in your brain—essentially turning up your nervous system’s natural brake pedal when mania is pushing the accelerator. It’s particularly effective for acute mania and shows moderate prophylactic benefits with median relapse-free survival around 36 months.
Common Side Effects
Gastrointestinal effects like nausea, vomiting, and indigestion affect 20-30% of people starting valproate. The extended-release formulation (Depakote ER) causes less stomach upset than immediate-release versions.
Tremor occurs in about 25% of people on valproate, similar to lithium. It’s usually dose-related and improves if your prescriber lowers the dose.
Weight gain is one of the most troublesome side effects, affecting 40-50% of people on valproate. The average gain is 10-15 pounds in the first year, but some people gain significantly more. Valproate appears to increase appetite and may alter metabolism.
Hair changes including hair loss or changes in hair texture happen to about 10% of people. Hair typically grows back, sometimes with a different texture (curlier or straighter than before). Taking zinc and selenium supplements may help, though the evidence is limited.
Sedation is common initially but usually improves after the first few weeks. Taking your full dose at bedtime can help you sleep through the drowsiness.
Serious Side Effects and Warnings
Liver toxicity is rare but potentially fatal. Your risk is highest in the first six months of treatment. Warning signs include unusual fatigue, weakness, facial swelling, loss of appetite, and vomiting. You need immediate medical evaluation if these develop.
Pancreatitis (inflammation of the pancreas) occurs in about 1 in 1,000 people taking valproate. Symptoms include severe abdominal pain, nausea, and vomiting. This is a medical emergency.
Polycystic ovary syndrome (PCOS) develops in 8-10% of women taking valproate, causing irregular periods, excess facial hair, acne, and fertility problems. The risk appears higher if you start valproate before age 20.
Thrombocytopenia (low platelet count) can cause easy bruising or bleeding. Your prescriber will monitor your platelet count with regular blood tests.
New Regulatory Restrictions (2024)
In 2024, regulatory agencies in multiple countries strengthened warnings about valproate use in women of childbearing potential due to high rates of birth defects (approximately 10% of pregnancies) and developmental delays in children exposed in utero. Many countries now require pregnancy prevention programs for anyone who could become pregnant while taking valproate.
If you’re someone who could become pregnant, your prescriber should discuss these risks thoroughly and ensure you’re using effective contraception if you take valproate. For many people, this has shifted prescribing patterns toward alternatives like lamotrigine for bipolar depression.
Monitoring Requirements
You’ll need baseline liver function tests and complete blood count before starting valproate, then follow-up tests at 2 weeks, 1 month, 3 months, and every 6-12 months thereafter. You’ll also need valproate level checks to ensure you’re in the therapeutic range (typically 50-125 mcg/mL).
Lamotrigine (Lamictal)
Lamotrigine stabilizes mood by blocking sodium channels in neurons, which prevents the excessive electrical activity that can trigger mood episodes. It’s particularly effective for bipolar depression and shows good prophylactic benefits for preventing depressive episodes. The clinical data shows response rates above 50% for moderate to severe bipolar depression.
Common Side Effects
Headache affects about 25% of people starting lamotrigine but usually resolves within a few weeks.
Nausea and dizziness occur in 15-20% of people, typically improving as your body adjusts.
Insomnia or sleep disturbances happen to about 10% of people. Taking lamotrigine in the morning rather than evening sometimes helps.
Blurred or double vision occurs rarely but should prompt a call to your prescriber.
The good news about lamotrigine is that it’s one of the most weight-neutral psychiatric medications—most people don’t experience significant weight changes. It also doesn’t typically cause cognitive dulling or sedation, making it more tolerable for many people than other mood stabilizers.
The Rash Warning — Understanding the Real Risk
Lamotrigine carries a black box warning about serious rashes, including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN)—potentially life-threatening conditions where your skin essentially burns from the inside out. This warning terrifies people, but understanding the actual risk helps you make informed decisions.
The serious rash risk is approximately 0.1% (1 in 1,000) when lamotrigine is titrated slowly according to the recommended schedule. The risk jumps to about 1% (1 in 100) if you increase the dose too quickly or if you’re taking valproate at the same time, which doubles lamotrigine blood levels.
Any rash on lamotrigine requires immediate medical evaluation—don’t wait to see if it gets better. Most rashes on lamotrigine are benign, but you can’t tell the difference between a harmless rash and a dangerous one without medical assessment.
Warning signs of a serious rash include rash accompanied by fever, blisters, peeling skin, rash involving your mouth or eyes, or rash that spreads rapidly. These require emergency medical care.
The slow titration schedule exists specifically to minimize rash risk. You’ll typically start at 25 mg daily for two weeks, then increase gradually over 6-8 weeks to reach a therapeutic dose. This feels frustratingly slow when you’re suffering from depression, but it’s the protocol that keeps the serious rash risk below 0.1%.
Monitoring
Lamotrigine doesn’t require regular blood level monitoring for most people, though your prescriber might check levels if you’re taking other medications that interact with lamotrigine or if you’re not responding as expected. You don’t need routine lab work for kidney or liver function with lamotrigine, making it lower-maintenance than lithium or valproate.
For a comprehensive overview of medication options and how they fit into your overall treatment plan, see our complete guide to bipolar disorder medications.
Atypical Antipsychotics: Side Effects by Class
Atypical antipsychotics work by blocking dopamine and serotonin receptors in your brain, which helps stabilize both manic and depressive episodes. Medications like quetiapine, olanzapine, aripiprazole, and risperidone show significant efficacy—quetiapine produces effect sizes of 0.54-0.61 on depression rating scales, and olanzapine achieves symptomatic remission in 70% of people with bipolar I mania.
But these medications come with a side-effect profile that requires careful monitoring and proactive management.
Metabolic Effects — The Most Clinically Important Concern
Weight gain is the most common and often most distressing side effect of atypical antipsychotics. The degree varies significantly by medication:
- Olanzapine causes the most weight gain, averaging 15-20 pounds in the first year, with some people gaining 40+ pounds
- Quetiapine causes moderate weight gain, typically 10-15 pounds
- Risperidone causes moderate weight gain, around 5-10 pounds
- Aripiprazole and lurasidone are more weight-neutral, with average gains under 5 pounds
The weight gain happens through multiple mechanisms: increased appetite, changes in metabolism, and alterations in how your body processes glucose and stores fat. For many people, the weight gain feels uncontrollable despite diet and exercise efforts.
Diabetes risk increases with atypical antipsychotics, particularly olanzapine and quetiapine. These medications can cause insulin resistance, where your body’s cells stop responding normally to insulin. Some people develop full type 2 diabetes. The risk is highest in people who gain significant weight, but metabolic changes can occur even without major weight gain.
Cholesterol and triglyceride increases occur in 20-40% of people on atypical antipsychotics. Elevated lipids increase your cardiovascular risk over time.
These metabolic effects are why baseline screening and ongoing monitoring are essential. You should have fasting glucose, hemoglobin A1c, lipid panel, weight, and waist circumference measured before starting an atypical antipsychotic, then rechecked at 4 weeks, 8 weeks, 12 weeks, and every 3-6 months thereafter.
If you develop significant weight gain or metabolic changes, your options include switching to a more weight-neutral antipsychotic, adding metformin (which can help with weight and insulin resistance), or intensifying diet and exercise interventions.
Sedation
Drowsiness and sedation are extremely common with atypical antipsychotics, especially quetiapine and olanzapine. For some people, this is actually helpful—if you’re experiencing insomnia during a manic episode, the sedation helps you sleep. But for others, the sedation persists beyond the acute phase and interferes with daily functioning.
The sedation usually improves somewhat over the first few weeks as your body adjusts. Taking your full dose at bedtime rather than splitting doses throughout the day can help you function better during the day. If sedation remains problematic after 4-6 weeks, your prescriber might lower your dose or switch you to a less sedating option like aripiprazole.
Movement-Related Side Effects (Extrapyramidal Symptoms)
Akathisia is a feeling of inner restlessness where you feel like you can’t sit still. It’s deeply uncomfortable—you might pace constantly, rock back and forth, or feel like you need to keep moving. Akathisia occurs in about 10-15% of people on atypical antipsychotics, more commonly with risperidone and aripiprazole than with quetiapine or olanzapine.
Akathisia often gets mistaken for anxiety or agitation, but it’s a medication side effect that requires intervention. Your prescriber might lower your dose, add a beta-blocker like propranolol, or switch you to a different medication.
Dystonia (muscle spasms or abnormal postures) and parkinsonism (tremor, stiffness, slowed movement) are less common with atypical antipsychotics than with older antipsychotics but still occur, particularly at higher doses.
Tardive dyskinesia is a late-onset movement disorder causing involuntary movements, typically of the face, mouth, and tongue. The risk with atypical antipsychotics is lower than with older antipsychotics (about 5% per year of exposure versus 20% with older drugs), but it’s not zero. The risk increases with longer duration of treatment and higher doses.
This is why your prescriber should check for abnormal movements at each visit using a standardized scale. If caught early, tardive dyskinesia may improve after stopping the medication, but in some cases it becomes permanent.
Other Common Antipsychotic Side Effects
Prolactin elevation occurs particularly with risperidone and can cause irregular periods, breast enlargement or discharge, sexual dysfunction, and bone density loss over time. Aripiprazole and quetiapine cause less prolactin elevation.
Sexual side effects including decreased libido, erectile dysfunction, and difficulty with arousal or orgasm affect 20-40% of people on antipsychotics. These effects are often underreported because people feel embarrassed discussing them, but they significantly impact quality of life and relationships.
Dry mouth, constipation, and blurred vision occur due to anticholinergic effects, particularly with quetiapine and olanzapine.
Monitoring for Atypical Antipsychotics
Beyond the metabolic monitoring mentioned earlier, you need regular assessment for movement disorders. Your prescriber should use a standardized tool like the Abnormal Involuntary Movement Scale (AIMS) at least every 6 months to screen for tardive dyskinesia.
You should also have blood pressure checks, as some antipsychotics can cause orthostatic hypotension (dizziness when standing up due to blood pressure drops).
Side Effects That Affect Adherence Most
Research on medication adherence in bipolar disorder consistently identifies several side effects as the primary reasons people stop taking their medications:
Weight gain ranks as the number one adherence barrier. The psychological impact of gaining 20, 30, or 40+ pounds affects self-esteem, body image, and physical health. Many people reach a point where they decide the mood stability isn’t worth the weight gain.
Cognitive effects—feeling mentally slowed, having difficulty concentrating, or experiencing memory problems—rank second. People describe feeling like they’re “not themselves” or like they’re “thinking through fog.” For people whose identity includes being sharp, articulate, or intellectually quick, cognitive dulling feels like losing a core part of who they are.
Sedation that persists beyond the first few weeks makes it difficult to work, care for children, or engage in activities you enjoy. When you’re sleeping 12 hours a day and still feel tired, the medication starts feeling like it’s stealing your life.
Sexual side effects profoundly impact intimate relationships and quality of life, yet people often don’t mention them to prescribers because of embarrassment or because they don’t realize the medication is causing the problem.
Tremor that interferes with work (especially if you do detailed manual tasks) or that makes you feel self-conscious in social situations becomes intolerable for many people.
The pattern is clear: side effects that affect your sense of self, your relationships, or your ability to function in valued roles are the ones most likely to make you stop taking medication. This is why the conversation about side effects needs to happen before you start a medication, not after you’ve already decided to stop taking it.
Understanding what to expect when you’re diagnosed with bipolar disorder includes preparing for these medication trade-offs from the beginning.
Managing Side Effects: General Principles
You have more options for managing side effects than you might realize. The key is addressing them proactively rather than suffering in silence until you can’t take it anymore.
Timing adjustments can make a significant difference. Taking sedating medications at bedtime rather than in the morning lets you sleep through the drowsiness. Taking medications with food reduces gastrointestinal side effects. Splitting doses throughout the day can minimize peak-level side effects.
Dose optimization matters enormously. Sometimes you’re taking more medication than you actually need for mood stability. Your prescriber might be able to lower your dose enough to reduce side effects while maintaining efficacy. This requires careful monitoring and honest communication about both your mood symptoms and side effects.
Medication switches become necessary when side effects are intolerable despite dose adjustments and management strategies. Switching from olanzapine to aripiprazole might resolve weight gain. Switching from lithium to lamotrigine might eliminate tremor and cognitive effects. The goal is finding the medication that provides the best balance of efficacy and tolerability for your specific situation.
Adjunctive medications can counteract specific side effects. Metformin helps with weight gain and insulin resistance from antipsychotics. Propranolol reduces tremor from lithium or valproate. Benztropine treats extrapyramidal symptoms. Modafinil or stimulants might help with sedation or cognitive effects, though this requires careful monitoring for mood destabilization.
Lifestyle interventions provide modest but meaningful benefits. Regular exercise helps counteract weight gain and improves mood independently. Protecting your sleep architecture—maintaining consistent sleep-wake times, creating a dark cool bedroom environment, limiting screens before bed—supports both mood stability and medication tolerability. Nutrition counseling can help you manage weight gain more effectively.
Monitoring and early intervention prevent small problems from becoming big ones. Catching a 5-pound weight gain early and addressing it is much easier than trying to reverse a 30-pound gain. Recognizing early signs of lithium toxicity prevents a medical emergency.
The principle underlying all of this is sustainable stability. You’re not looking for perfect—you’re looking for a management protocol you can maintain long-term that keeps you functionally stable. That means finding the side-effect trade-off you can live with, not the one that looks best on paper.
For more strategies on managing the daily realities of bipolar disorder, including medication side effects, see our guide on living with bipolar disorder.
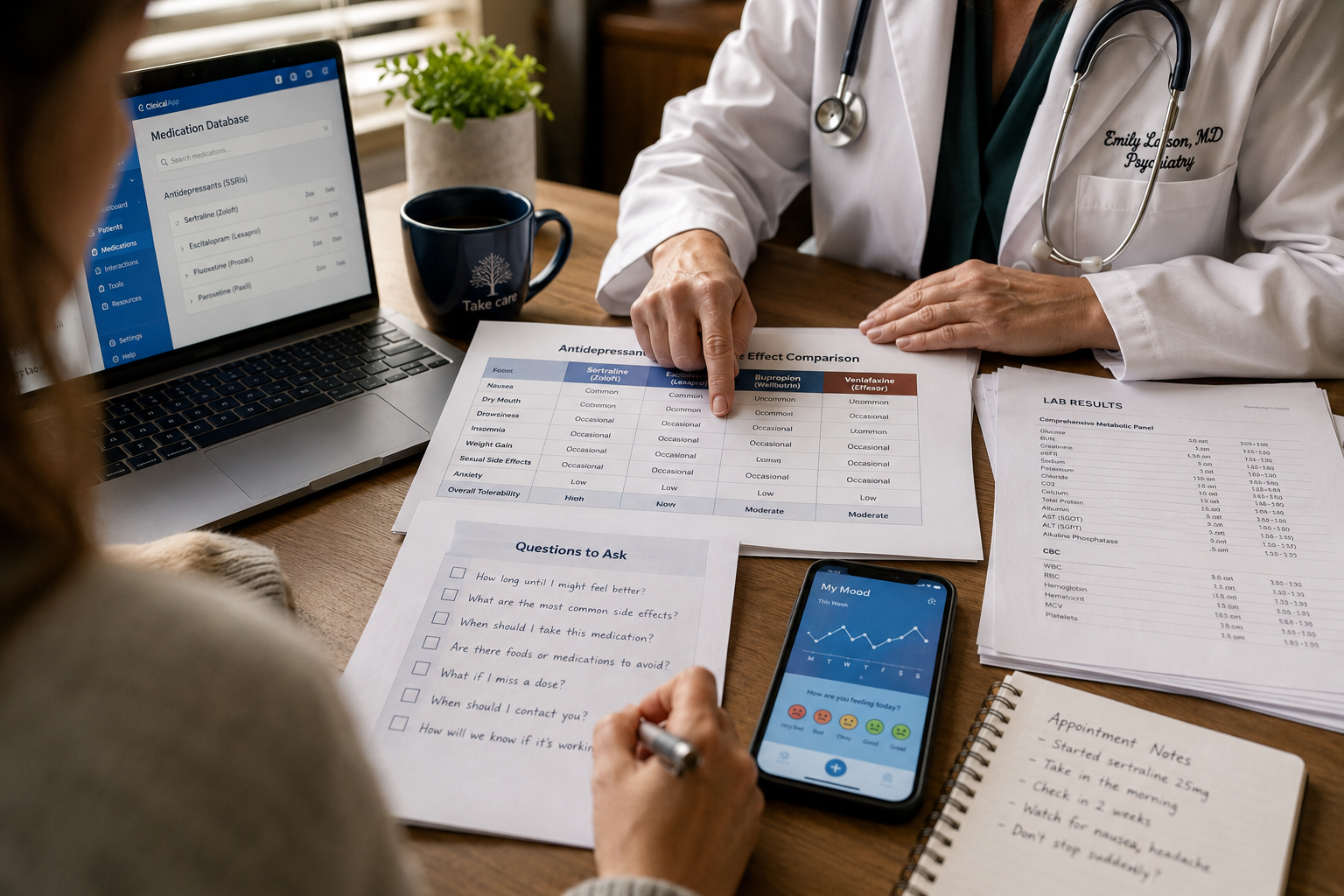
Questions to Ask Your Prescriber About Side Effects
Before starting any new medication, you deserve clear answers to these questions:
What are the most common side effects of this medication, and when do they typically appear? You need to know what to expect in the first few days, the first few weeks, and over months of treatment.
Which side effects should prompt me to call you immediately versus which ones can wait until my next appointment? Understanding the difference between concerning and expected side effects reduces anxiety and ensures you get help when you actually need it.
What’s your plan for monitoring side effects? Ask specifically about blood work, weight checks, movement disorder screening, and metabolic monitoring. If your prescriber doesn’t mention monitoring, that’s a red flag.
If I develop [specific side effect you’re concerned about], what are our options? Having a plan in advance for managing the side effects you’re most worried about makes you more likely to actually report them if they occur.
How long should I try this medication before we consider it a failure? You need to know the timeline for both therapeutic effects and side effects. Some side effects improve after a few weeks; others persist or worsen.
What are the alternatives if this medication doesn’t work or causes intolerable side effects? Knowing you have options reduces the pressure to make any single medication work.
How does this medication interact with my other medications or medical conditions? Drug interactions and medical comorbidities significantly affect side effect risk.
What should I do if I miss a dose? Knowing the protocol in advance prevents panic and poor decisions.
What’s the process for stopping this medication if we need to? Some medications require gradual tapering to avoid withdrawal effects or rebound mood episodes.
How will we know if this medication is working? Defining success criteria in advance—specific mood symptoms improving, functioning better at work, sleeping more consistently—helps you and your prescriber evaluate whether the medication is worth the side effects.
These questions shift the conversation from passive acceptance of whatever your prescriber recommends to active collaboration in finding the right treatment protocol for you. You’re the expert on your own body and your own life—your prescriber is the expert on medications. Treatment works best when you combine both types of expertise.
If you’re supporting someone with bipolar disorder through medication decisions, our guide on how to help your partner manage their bipolar disorder offers practical strategies for being supportive without being controlling.
Charting Your Next Baseline
The side-effect trade-off is real, and pretending otherwise doesn’t help anyone. Every medication that stabilizes your mood comes with physical effects, and finding sustainable stability means finding the balance you can maintain long-term.
Here’s what matters most: you don’t have to accept intolerable side effects. If weight gain is destroying your self-esteem, if cognitive effects are interfering with your work, if sedation is stealing your life, or if sexual side effects are damaging your relationship, those are legitimate reasons to work with your prescriber on adjusting your treatment protocol.
But you also don’t have to make these decisions alone or in crisis. Start with a mood tracking inventory that captures both your mood symptoms and any side effects you’re experiencing. Track your earliest warning sign of both mood episodes and medication problems. This data becomes the foundation for informed conversations with your prescriber about whether your current protocol is working or whether you need adjustments.
The goal isn’t finding a medication with zero side effects—that medication doesn’t exist. The goal is finding the medication that gives you the most mood stability with side effects you can manage, then building a comprehensive management protocol around that foundation.
That protocol includes medication, yes, but also therapy, sleep protection, nervous system regulation strategies, social support, and trigger-and-response planning. Medication is the foundation for most people with bipolar disorder, but it’s not the entire structure.
Your true baseline—the version of yourself that’s stable, functional, and genuinely you—is worth fighting for. That fight includes advocating for yourself when side effects become intolerable, staying engaged with treatment even when it’s frustrating, and remembering that finding the right protocol often takes time and multiple adjustments.
You’re not failing if the first medication doesn’t work or causes side effects you can’t tolerate. You’re gathering data about what your body needs and what it can’t handle. Each medication trial, each dose adjustment, each side effect managed or medication switched brings you closer to sustainable stability.
The decades of clinical data show that people with bipolar disorder who stay engaged with treatment, work collaboratively with their prescribers, and find a medication protocol they can maintain long-term have dramatically better outcomes than those who cycle through medications without addressing side effects or who give up on treatment entirely.
You deserve both mood stability and quality of life. When those two goals conflict, you deserve a prescriber who takes both seriously and works with you to find solutions. If your current prescriber dismisses your side effect concerns or tells you to just deal with it, you deserve a different prescriber.
The path to sustainable stability isn’t linear, and it’s rarely quick. But it’s possible, and understanding bipolar disorder medication side effects is an essential part of that journey.
Frequently Asked Questions
How long do medication side effects typically last?
Most side effects follow one of three patterns: some appear immediately and fade within 2-4 weeks as your body adjusts (nausea, initial sedation), others develop gradually over months (weight gain, metabolic changes), and a few require immediate attention regardless of timing (serious rash, signs of toxicity).
If a side effect persists beyond 4-6 weeks and significantly affects your functioning, contact your prescriber about adjustments rather than waiting to see if it improves.
Can I prevent weight gain from bipolar medications?
You can’t completely prevent weight gain from medications like olanzapine or quetiapine, but you can minimize it through early intervention. Start monitoring your weight weekly from day one, work with a nutritionist familiar with psychiatric medication effects, maintain regular exercise, and address even small gains immediately.
Some people benefit from adding metformin, which can reduce weight gain by 5-10 pounds on average. Switching to more weight-neutral options like aripiprazole or lamotrigine is sometimes necessary.
What should I do if I experience sexual side effects from my medication?
Talk to your prescriber specifically about sexual side effects—they won’t know unless you tell them, and these effects significantly impact quality of life and medication adherence.
Options include lowering your dose, switching to a medication with lower sexual side effect rates (like lamotrigine or aripiprazole), adding medications that counteract sexual dysfunction, or timing doses to minimize impact on sexual activity. Don’t suffer in silence or stop your medication without discussing alternatives first.
Is it safe to stop taking my medication if the side effects are unbearable?
Never stop bipolar medications abruptly without medical guidance, as sudden discontinuation can trigger severe mood episodes or withdrawal effects. If side effects are truly unbearable, contact your prescriber immediately—same day if possible—to discuss either rapid tapering with bridge medication or emergency alternatives. Most prescribers can see you quickly for urgent medication concerns, and many have after-hours protocols for medication crises.
How do I know if a side effect is dangerous versus just uncomfortable?
Dangerous side effects requiring immediate medical attention include: any rash with fever or blisters, signs of lithium toxicity (severe tremor, confusion, vomiting), severe abdominal pain, chest pain or irregular heartbeat, sudden vision changes, signs of infection with low white blood cell count, or thoughts of self-harm.
Uncomfortable but non-emergency side effects include mild tremor, moderate weight gain, dry mouth, or mild sedation—these warrant a call to your prescriber within a few days but don’t require emergency care.
Can I take supplements to reduce medication side effects?
Some supplements show modest benefits for specific side effects: omega-3 fatty acids may help with mood and metabolic effects, zinc and selenium might reduce valproate-related hair loss, and vitamin D supports overall health. However, supplements can interact with bipolar medications—St. John’s wort can trigger mania, and some supplements affect medication blood levels.
Always discuss supplements with your prescriber before starting them, and don’t use supplements as a substitute for addressing intolerable side effects through medication adjustments.
Conclusion
Understanding and managing bipolar disorder medication side effects is essential for achieving sustainable stability. The medications that stabilize your mood—lithium, valproate, lamotrigine, and atypical antipsychotics—all come with side-effect profiles that require informed decision-making, proactive monitoring, and honest communication with your prescriber.
The key principles are straightforward: know what to expect before you start a medication, recognize which side effects require immediate attention versus which ones may improve with time, advocate for yourself when side effects become intolerable, and remember that finding the right medication protocol often requires adjustments and sometimes multiple trials.
Your next steps are concrete: if you’re considering starting a bipolar medication, use the questions in this article to have an informed conversation with your prescriber. If you’re already taking medication and experiencing side effects, document them specifically in your mood tracking inventory and schedule an appointment to discuss management options.
If side effects have made you consider stopping your medication, reach out to your prescriber before making that decision—alternatives exist that you may not have tried yet.
For comprehensive information about all aspects of bipolar disorder treatment, including medication options, therapy approaches, and lifestyle strategies, explore our complete bipolar disorder treatment guide. You can also find support and practical tools through our bipolar disorder support resources.
The path to sustainable stability requires patience, persistence, and partnership with your healthcare team. Side effects are real, but so are solutions—and you deserve both mood stability and quality of life.