Living With Bipolar Disorder: What Actually Helps Day to Day
You’re not failing at managing bipolar disorder because you lack willpower. You’re exhausted because the condition demands a level of self-monitoring that most people never have to think about, and nobody handed you the actual instruction manual when you got diagnosed with bipolar.
The clinical research shows that sustainable stability comes from matching specific interventions to your unique polarity pattern, not from generic advice about “staying positive.”
Living with bipolar disorder means learning a new language: the vocabulary of your own nervous system. You’ll discover that what works brilliantly during a depressive episode can backfire spectacularly during hypomania, and that the right med for the wrong cycle creates more problems than it solves.
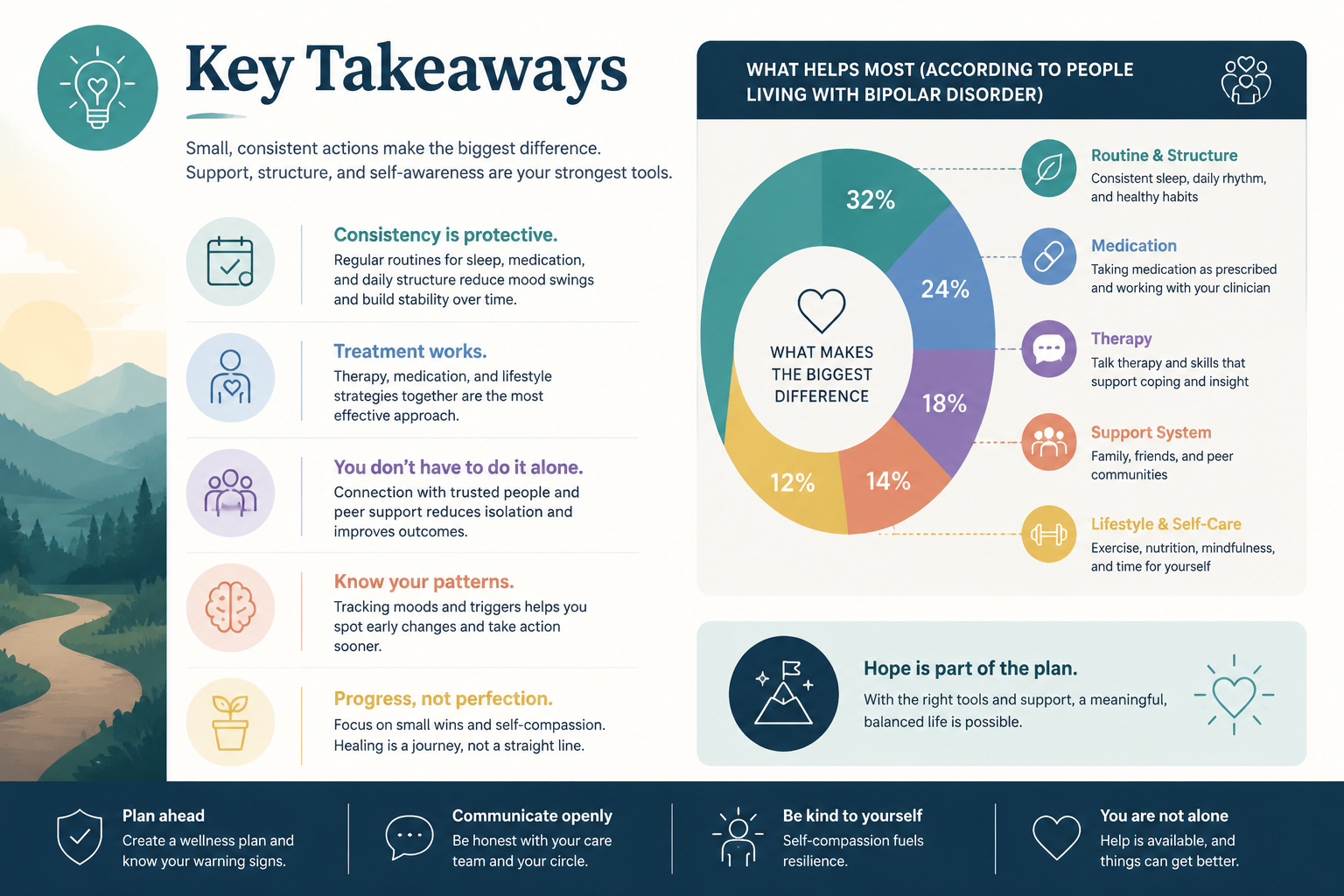
Key Takeaways
- Coping isn’t about eliminating symptoms—it’s about building cycle awareness before treatment selection and recognizing your earliest warning signs before episodes fully develop.
- Sleep architecture protection matters more than any single medication—disrupted sleep both triggers and worsens mood episodes, making consistent sleep timing non-negotiable.
- Sustainable stability requires matching interventions to your specific episode type—what stabilizes depression (like increased activity) can destabilize mania, demanding a flexible management protocol.
- Your support system needs clear instructions—healthy boundaries protect both you and your relationships when you define specific, actionable requests during stable periods.
- Long-term success looks like smaller swings, not perfect flatness—you’re aiming for a tighter range around your true baseline, not the elimination of all mood variation.
What “Coping” Really Means With Bipolar Disorder
Coping isn’t white-knuckling your way through episodes or pretending everything’s fine when your brain’s reward circuitry is stuck holding down the accelerator. It’s the systematic process of building a mood tracking inventory so detailed that you spot pattern shifts three days before anyone else notices.
You’re learning to read your own data. When you track sleep duration, social energy, spending impulses, and irritability on a simple 1-10 scale for ninety days, your polarity pattern emerges like a photograph in developing fluid—you’ll see whether you cycle with the seasons, whether mixed episodes sneak in after stress, whether your baseline tilts more toward depression or activation.
The decades of clinical data are clear: people who understand their trigger-and-response patterns before selecting treatments have better outcomes than those who start with medication trials and hope for the best. Cycle awareness before treatment selection isn’t just smart—it’s the difference between throwing darts blindfolded and actually hitting the target.
Accepting the Diagnosis Without Letting It Define You
The diagnosis explains why your brain does what it does. It doesn’t tell you who you are or what you’re capable of becoming.
You’ll notice something strange in the first year after diagnosis: some people treat bipolar disorder like a personality trait (“I’m so bipolar!”), while others refuse to acknowledge it exists. Neither extreme serves you well—the first collapses your entire identity into a medical condition, the second leaves you vulnerable because you won’t prepare for what’s coming.
Here’s what acceptance actually looks like in plain English: you acknowledge that your nervous system requires specific maintenance protocols, the same way someone with diabetes monitors blood sugar.
You’re not broken, you’re not damaged, and you’re certainly not less capable—you’re someone whose brain chemistry needs active management to function at its best. That management becomes part of your routine, like brushing your teeth, not the central drama of your existence.
Understanding What Bipolar Disorder Actually Affects in Your Life
Bipolar disorder doesn’t just shift your mood—it recalibrates your entire relationship with energy, sleep, decision-making, and social connection. When your brain’s mood regulation system misfires, the ripple effects touch everything from how you experience pleasure to how you assess risk.
During depressive episodes, your brain’s reward circuitry essentially goes offline. Activities that used to bring joy feel hollow, your body feels physically heavier, and your thinking slows to the point where simple decisions become exhausting.
You’re not lazy or unmotivated—your dopamine signaling has temporarily crashed, making it neurologically difficult to initiate action or feel satisfaction.
Mania and hypomania flip the script entirely. Your brain floods with dopamine and norepinephrine, creating a sensation of limitless energy and confidence that feels incredible until it doesn’t. Sleep feels optional, ideas cascade faster than you can capture them, and your usual risk assessment disappears—which is why people make impulsive financial decisions, start projects they’ll never finish, or damage relationships with uncharacteristic irritability.
The cognitive effects persist even between episodes. Many people with bipolar disorder experience subtle difficulties with working memory, attention, and executive function that make complex tasks harder than they should be. This isn’t permanent brain damage—it’s more like background static that requires extra effort to filter out.
Understanding these mechanisms helps you separate yourself from your symptoms. When you recognize that your sudden urge to reorganize your entire life at 2 AM is dopamine dysregulation rather than genuine inspiration, you can pause before acting on it.
Building Stability: The Foundation of Coping
Stability doesn’t emerge from a single intervention—it’s constructed from multiple layers of protection that work together to keep your nervous system regulated. You’re building a foundation that can withstand the inevitable stressors and disruptions that trigger mood episodes.
Sleep as Medicine, Not Lifestyle
Your sleep architecture is the single most powerful lever you have for mood stability. When you sleep, your brain clears metabolic waste, consolidates memories, and recalibrates neurotransmitter systems—all processes that directly affect mood regulation.
Here’s what the research shows: even one night of sleep deprivation can trigger manic symptoms in vulnerable individuals, while chronic sleep disruption predicts depressive episodes. Your circadian rhythm and your mood regulation system are so tightly linked that protecting one automatically protects the other.
Protect your sleep architecture means going to bed and waking up at the same time every single day, including weekends. Your brain’s internal clock needs consistency to function properly—shifting your sleep schedule by even two hours creates a mini jet-lag effect that destabilizes mood. You’re aiming for 7-9 hours in a dark, cool room, with screens off an hour before bed and no caffeine after 2 PM.
When hypomania starts eroding your sleep, that’s your earliest warning sign that an episode is building. You’ll need to intervene immediately with your management protocol rather than enjoying the temporary energy boost.
Routine as Protection
Routine sounds boring until you realize it’s the scaffolding that holds your nervous system steady when everything else is shifting. People living with bipolar disorder benefit enormously from structured daily rhythms—not because routine is inherently therapeutic, but because unpredictability and disruption are destabilizing.
Your routine should anchor around non-negotiable elements: consistent meal times, regular physical activity at the same time each day, predictable social contact, and structured work or purposeful activity. This isn’t about rigidity—it’s about creating enough predictability that your nervous system can relax instead of constantly scanning for threats.
Interpersonal and social rhythm therapy formalizes this approach by helping you identify which daily rhythms most affect your mood stability. You’ll track when you eat, sleep, exercise, and interact with others, then work to stabilize those patterns before adding other interventions.
The side-effect trade-off here is minimal: the only “cost” of routine is reduced spontaneity, which matters far less than preventing a full manic or depressive episode that derails your life for weeks or months.
Nutrition and Daily Physical Habits
Your brain runs on glucose, amino acids, and fatty acids—the raw materials that build neurotransmitters and maintain cellular function. When you skip meals, load up on processed carbohydrates, or yo-yo between restriction and bingeing, you’re adding unnecessary stress to a system that’s already working overtime to maintain stability.
You don’t need a perfect diet. You need consistent, adequate nutrition that keeps your blood sugar stable and provides the building blocks your brain needs. That means eating protein at every meal, including healthy fats, and avoiding the blood sugar roller coaster that comes from high-sugar, low-fiber foods.
Physical activity works as a mood stabilizer through multiple mechanisms: it improves insulin sensitivity, promotes neuroplasticity, regulates stress hormones, and provides structured routine. The research shows that moderate exercise (30 minutes of walking, cycling, or swimming most days) reduces both depressive and manic symptoms when maintained consistently.
The key word is moderate—intense exercise can be activating in ways that trigger hypomania in some people, while complete inactivity worsens depression. You’re looking for sustainable movement that you can maintain regardless of your mood state, not punishing workouts that you’ll abandon during episodes.
Managing Episodes When They Come
Even with perfect prevention, episodes will still occur. Your goal isn’t to eliminate them entirely—it’s to catch them earlier, reduce their severity, and recover faster by matching your response to the specific type of episode you’re experiencing.
Recognizing Your Personal Prodrome
Your earliest warning sign is the shift that happens before anyone else notices, sometimes days or weeks before a full episode develops. For some people, it’s a change in sleep need—suddenly feeling rested on five hours or unable to get out of bed despite ten. For others, it’s subtle shifts in social desire, irritability, spending patterns, or the speed of their thoughts.
You learn your prodrome by tracking consistently during stable periods and then looking back when episodes emerge. What changed first? What happened three days before you realized something was wrong? That pattern becomes your early detection system.
Common prodromal signs for mania include decreased sleep need, increased goal-directed activity, racing thoughts, heightened irritability, and increased spending or risk-taking. For depression, watch for increased sleep need, social withdrawal, loss of interest in previously enjoyable activities, difficulty concentrating, and physical heaviness.
The moment you spot your prodrome, you activate your management protocol—not next week, not after you “see how it goes,” but immediately.

What to Do When You Spot Warning Signs
Your management protocol is the specific set of actions you take when you recognize warning signs, customized to whether you’re heading toward depression or activation. You create this protocol during stable periods, when your judgment is clear, so you don’t have to make decisions when your brain chemistry is already shifting.
For emerging mania or hypomania, your protocol might include: immediately returning to strict sleep schedule with medication if needed, reducing stimulation (less social activity, no new projects, limited screen time), increasing structure and routine, contacting your prescriber about medication adjustment, and asking your support system to help monitor your behavior.
For emerging depression, you might: maintain minimum activity levels even when motivation disappears, increase social contact even briefly, ensure adequate light exposure especially in morning, stick to routine even when it feels pointless, and contact your therapist or prescriber for intervention.
The key is having these protocols written down and shared with your support system before you need them. When you’re in the early stages of an episode, your insight often diminishes—you might not recognize that your “great ideas” are actually hypomanic grandiosity, or that your “need for rest” is depression pulling you under.
During a Depressive Episode
When you’re in a full depressive episode, your goal shifts from prevention to harm reduction and maintaining minimum function. You’re not trying to feel good—you’re trying to prevent the episode from deepening and to maintain the basic structure that will help you recover.
Maintain your routine even when it feels mechanical and pointless. Your brain needs the external structure because its internal regulation system is offline. Get out of bed at your regular time, eat meals at consistent times, and move your body even if it’s just a ten-minute walk. These actions won’t cure the depression, but they prevent the downward spiral that happens when you surrender completely to the episode.
Increase your treatment intensity if needed. This might mean more frequent therapy sessions, medication adjustment, or adding evidence-based interventions like bright light therapy or behavioral activation. The research shows that psychotherapy helps treat bipolar disorder particularly during depressive episodes, when cognitive and behavioral interventions can interrupt negative thought patterns and restore activity levels.
Protect yourself from major decisions. Depression distorts your thinking in predictable ways—everything feels hopeless, permanent, and catastrophic. Don’t quit your job, end relationships, or make other irreversible choices during episodes. These decisions almost always look different once the episode lifts.
During Mania or Hypomania
Mania is trickier because it often feels good, at least initially. You have energy, confidence, and creativity that seem like gifts rather than symptoms. The challenge is recognizing that these states are unsustainable and typically end in either a crash into depression or consequences from impulsive decisions made during activation.
Reduce stimulation immediately. This means cutting back on social activities, avoiding new projects or commitments, limiting screen time especially late at night, and creating a calm environment. Your nervous system is already overstimulated—adding more input makes it worse.
Protect your sleep by any means necessary. This might require medication adjustment, strict sleep hygiene, or even short-term use of sedating medications to ensure you’re getting adequate rest. Sleep deprivation during mania creates a vicious cycle where lack of sleep worsens mania, which further disrupts sleep.
Implement spending controls before you need them. Give your credit cards to someone you trust, set up account alerts for transactions over a certain amount, or freeze your credit. Impulsive spending during mania can create financial consequences that last long after the episode ends.
Increase monitoring and accountability. You need people around you who can provide reality checks when your judgment is impaired. This might mean daily check-ins with a family member, more frequent appointments with your treatment team, or asking someone to help you evaluate decisions before you act on them.
If you’re experiencing full mania with psychotic features, delusions, or severely impaired judgment, you may need hospitalization. This isn’t failure—it’s appropriate medical care for a serious episode that requires intensive treatment.
Working With Your Support System
You can’t manage bipolar disorder entirely alone, but you also can’t expect others to read your mind or know instinctively what you need. Building an effective support system means being specific about what helps, what doesn’t, and what you need from different people in your life.

What to Ask of the People Around You
The people who care about you want to help, but they often don’t know how. Your job is to give them clear, specific instructions during stable periods so they know what to do when episodes emerge.
You might ask your partner or close family member to: monitor your sleep patterns and alert you when they notice changes, help you stick to routine when motivation disappears, provide reality checks when your judgment seems impaired, attend appointments with you when needed, and manage finances during manic episodes.
You might ask friends to: maintain regular contact even when you withdraw, invite you to low-key activities during depression, gently redirect you when you’re oversharing or overstimulated, and not take it personally when you need space.
You might ask your coworkers or manager to: allow flexible scheduling when possible, understand that you may need occasional mental health days, and maintain normal expectations and interactions rather than treating you differently.
The key is specificity. “Be supportive” is too vague. “Text me every morning during depressive episodes even if I don’t respond, and help me get out of the house at least twice a week” gives people actionable guidance.
What Healthy Boundaries Look Like for You
Boundaries protect both you and your relationships. They’re not about pushing people away—they’re about creating sustainable structures that prevent burnout and resentment on both sides.
You need boundaries around: how much you share about your symptoms (not everyone needs detailed updates), what you’re willing to accept from others (support yes, enabling no), how much responsibility others can take for your management (they can help, but you’re ultimately in charge), and what happens during episodes (predetermined agreements about decision-making, finances, or crisis intervention).
Healthy boundaries mean you don’t expect others to fix your disorder or manage your emotions for you. You take responsibility for following your treatment plan, communicating your needs clearly, and doing the daily work of stability. In return, you ask for specific, reasonable support rather than constant caretaking.
You also need boundaries that protect you from people or situations that destabilize your mood. This might mean limiting contact with family members who dismiss your diagnosis, avoiding friends who encourage risky behavior during hypomania, or stepping back from high-stress commitments that trigger episodes.
How to help your partner manage their bipolar disorder offers guidance for the people supporting you, helping them understand what effective support looks like versus unhelpful patterns that create dependency or conflict.
The Long View: What Living Well With Bipolar Actually Looks Like
Living well with bipolar disorder doesn’t mean achieving perfect stability or never experiencing symptoms. It means building a life where episodes become less frequent, less severe, and less disruptive—where you recover faster and maintain more of your functioning even during difficult periods.
Your true baseline is probably different from what you imagined before diagnosis. You’re not aiming for the sustained euphoria of hypomania or the flat emotional state that some medications can create. You’re looking for a range of normal human emotions and energy levels, with smaller fluctuations that don’t derail your life.
Sustainable stability looks like: recognizing warning signs early and intervening before full episodes develop, maintaining your routine and treatment plan even when you feel good, having a support system that understands your needs, making decisions that protect your stability rather than chasing short-term excitement, and accepting that some days will be harder than others without catastrophizing.
You’ll learn to distinguish between normal mood variation and the beginning of an episode. Everyone has good days and bad days, periods of higher and lower energy, times when they’re more or less social. The difference is that your nervous system can amplify these normal variations into something more extreme if you’re not paying attention.
The research on bipolar disorder medications shows that lithium offers the strongest prophylactic benefits for bipolar I, with median relapse-free survival reaching 81 months compared to shorter durations with other mood stabilizers. But medication is just one piece—your daily habits, self-awareness, and support system matter just as much for long-term outcomes.
You’ll also discover that living with bipolar disorder gives you certain advantages: heightened emotional sensitivity that deepens relationships when managed well, creativity and energy during hypomanic periods that you can channel productively, and profound self-knowledge that comes from years of tracking your own patterns. These aren’t consolation prizes—they’re real strengths that emerge when you’re not constantly fighting against your disorder.
Success means building a life that accommodates your needs rather than constantly pushing against them. You choose careers with flexibility rather than rigid schedules, relationships with people who understand your condition, and lifestyles that prioritize stability over constant novelty. These aren’t limitations—they’re informed choices that let you thrive rather than just survive.
Charting Your Next Baseline
You’re not starting from scratch. You already know more about your patterns than you did six months ago, and you’ll know even more six months from now. Each episode teaches you something—what your warning signs look like, which interventions work, what triggers to avoid, how long recovery takes.
Your next step is creating or refining your mood tracking inventory. Start with a simple daily log: sleep hours, mood rating, energy level, irritability, social desire, and any significant events or stressors. Track for at least ninety days to see patterns emerge. You’re looking for your polarity pattern—do you cycle with seasons, stress, hormones, or no obvious trigger?
Once you understand your pattern, you can build your management protocol. Write down specifically what you’ll do when you spot warning signs of depression versus mania. Share this protocol with your support system and your treatment team. Update it as you learn what works and what doesn’t.
If you’re not already working with a psychiatrist experienced in treating bipolar disorder, that’s your priority. Medication management requires expertise in matching compounds to your specific presentation, adjusting doses as needed, and managing the side-effect trade-offs that come with every intervention.
Consider adding talk therapy to your treatment plan if you haven’t already. Cognitive-behavioral therapy, interpersonal and social rhythm therapy, and family-focused therapy all have strong evidence for improving outcomes in bipolar disorder. Therapy gives you tools for managing symptoms, processing the emotional impact of the diagnosis, and building the self-awareness that makes everything else work better.
Connect with others who understand what you’re going through. Support groups provide validation, practical advice, and the reminder that you’re not alone in this experience. Hearing how others manage their symptoms often sparks ideas you wouldn’t have discovered on your own.
Most importantly, give yourself credit for the work you’re already doing. Managing bipolar disorder requires daily effort that most people never have to think about. You’re learning to read your own nervous system, building stability through routine and treatment, and making choices that protect your long-term wellbeing even when they’re not the most exciting options. That’s not just coping—that’s genuine skill and strength.
Frequently Asked Questions
How long does it take to stabilize after a bipolar diagnosis?
Stabilization is a process, not a destination. Most people see significant improvement within 3-6 months of starting appropriate treatment, but finding the right medication combination and building effective routines often takes a year or more. You’re looking for a gradual reduction in episode frequency and severity rather than immediate perfect stability.
Can you live a normal life with bipolar disorder?
Yes, with appropriate treatment and management. Many people with bipolar disorder maintain successful careers, relationships, and families. “Normal” looks different for everyone—your version includes medication management, routine protection, and ongoing self-monitoring, but these become background habits rather than constant struggles.
What’s the difference between a bad day and the start of an episode?
Bad days are temporary, proportional to circumstances, and don’t include your personal prodromal signs. Episodes involve multiple symptoms clustering together, changes in sleep or energy that persist for several days, and the specific warning signs you’ve learned to recognize in your own pattern. When in doubt, treat it as a potential episode and activate your management protocol.
Should I tell people I have bipolar disorder?
This depends entirely on the relationship and context. Close family and partners generally need to know so they can provide appropriate support. Employers and casual acquaintances don’t need details about your diagnosis. Share strategically with people who need to know to help you, and maintain privacy with those who don’t.
What do I do if my medication stops working?
Contact your prescriber immediately. Medication effectiveness can change over time due to tolerance, life changes, or shifts in your disorder’s presentation. Your doctor can adjust doses, add adjunctive medications, or switch to different compounds. Don’t stop taking medication abruptly or try to manage breakthrough symptoms alone.
How do I know if I need to go to the hospital?
Seek immediate care if you’re experiencing: suicidal thoughts with a plan, psychotic symptoms like delusions or hallucinations, severe mania with dangerous impulsivity, or complete inability to care for yourself. When in doubt, err on the side of getting evaluated—that’s what emergency services are for.
Conclusion
Living with bipolar disorder demands more self-awareness and daily maintenance than most people ever develop, but that intensive self-knowledge becomes your greatest asset. You’re learning to read your own patterns, match interventions to your specific needs, and build a life structure that supports stability rather than constantly threatening it.
The path forward isn’t about achieving perfect mood stability or eliminating all symptoms. It’s about catching episodes earlier, reducing their impact, maintaining your functioning during difficult periods, and building longer stretches of baseline stability between episodes. Each cycle teaches you something new about your triggers, your warning signs, and what actually helps versus what just sounds good in theory.
Start where you are. If you’re newly diagnosed, focus on building your mood tracking inventory and finding a treatment team you trust. If you’ve been managing for years, refine your protocols based on what you’ve learned. If you’re in an episode right now, focus on harm reduction and maintaining minimum structure until it passes.
You’re not alone in this, even when it feels isolating. Thousands of people are doing this same daily work, learning the same hard lessons, and building lives that work despite—and sometimes because of—their bipolar disorder. Your job is to keep learning, keep adjusting, and keep moving toward your version of sustainable stability.