
After Psychiatric Hospitalization: Returning Home and Rebuilding Stability (Bipolar Disorder)
The period after psychiatric hospitalization bipolar disorder treatment is not “the end of the episode”—it’s a high-vulnerability transition where the goal is to convert short-term inpatient stabilization into long-term stability at home. Reintegration is often best understood as a journey that shifts from institutional care toward self-management and supports in the community.
Source: The Reintegration Journey Following a Psychiatric Hospitalization (PMC) https://pmc.ncbi.nlm.nih.gov/articles/PMC9140300/
The Transition Home Is Its Own Clinical Risk
Why this period is dangerous (and why naming that risk helps)
Inpatient units reduce immediate danger and acute symptom intensity, but they can’t remove the real-world triggers waiting at home: sleep disruption, relationship stress, work pressure, substance access, or isolation. Reintegration research emphasizes that leaving the hospital changes the demands on you quickly—suddenly you are doing the regulating, scheduling, and monitoring that the unit temporarily handled.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC9140300/
This isn’t meant to scare you. It’s meant to justify taking the post-discharge window seriously and building a plan that is concrete, specific, and easy to follow when your brain is still recovering.
Why discharge doesn’t mean stable
Discharge often means:
- You’re safe enough to leave inpatient care
- A medication plan has started (not necessarily fully “working” yet)
- The immediate crisis has calmed enough for outpatient treatment to take over
But your baseline routines, sleep, and stress tolerance may still be fragile—especially in bipolar disorder, where rhythm disruption (sleep/wake timing, stimulation, social demands) can trigger mood instability.
Before You Leave the Hospital: What You Need
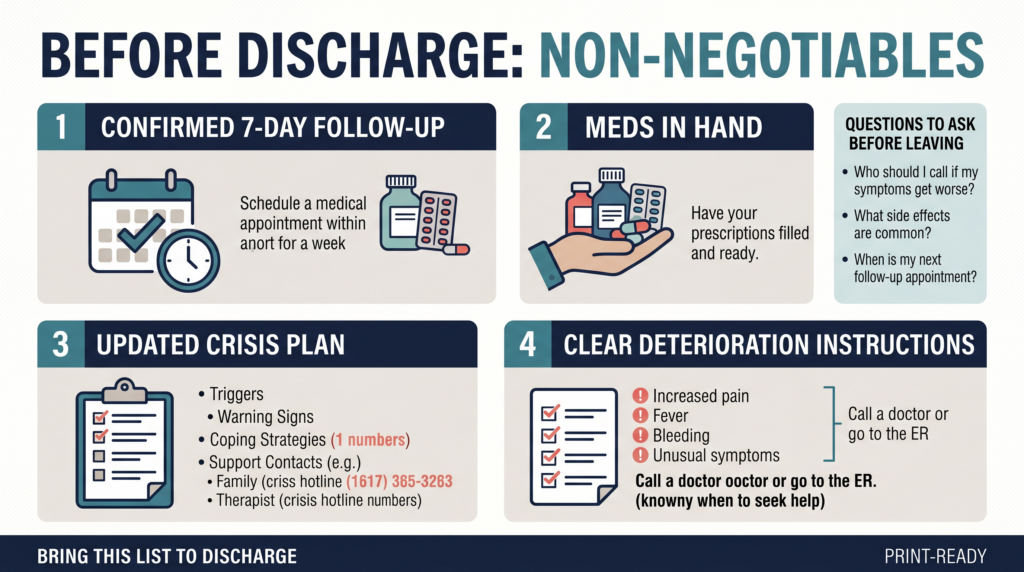
Non-negotiable before discharge
1) A follow-up appointment that is confirmed
“Call to schedule” is not a plan. You want a date/time appointment on paper (or in the portal) before you walk out, because the early days at home are when people most commonly fall through gaps.
2) Prescriptions filled and in hand
A smooth medication bridge matters because any delay, confusion, or missed doses can destabilize sleep and mood. Confirm:
- What you’re taking now
- What changed
- What time of day to take it
- What side effects are urgent vs. expected
3) Crisis plan updated
Use your hospitalization to update what you now know:
- Your earliest warning signs
- What helps you de-escalate
- Who should be contacted first
- Which ER you would go to (and how you’ll get there)
4) Clear instructions for deterioration
Ask this directly before discharge:
- “What should I do if my symptoms worsen before my follow-up?”
And get: - A specific number to call
- A specific service (clinic/on-call/triage line)
- Clear guidance about when to go to the ER
A practical discharge checklist for the transition home also emphasizes having a clear aftercare plan, medication continuity, scheduled follow-ups, and a safe environment.
Source: Transition from Psychiatric Hospital to Home: A Guide https://www.embarkbh.com/resources/parenting/transition-from-psychiatric-hospital-home/
Questions to ask before leaving
- What is my confirmed follow-up appointment?
- What meds am I taking now, and what changed?
- What side effects should I watch for?
- What symptoms mean I should go to the ER before my appointment?
- What should I not do in the first week?
The First 48–72 Hours at Home
This is often the hardest part
Going from a structured unit to home can feel jarring: too quiet, too open-ended, too many decisions. Reintegration literature describes this shift as moving from clinician-led structure to self-management, which can be challenging even when you want to recover.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC9140300/
Tell one trusted person how you’re doing during this window—especially if you feel “weird,” flat, agitated, ashamed, restless, or emotionally flooded.
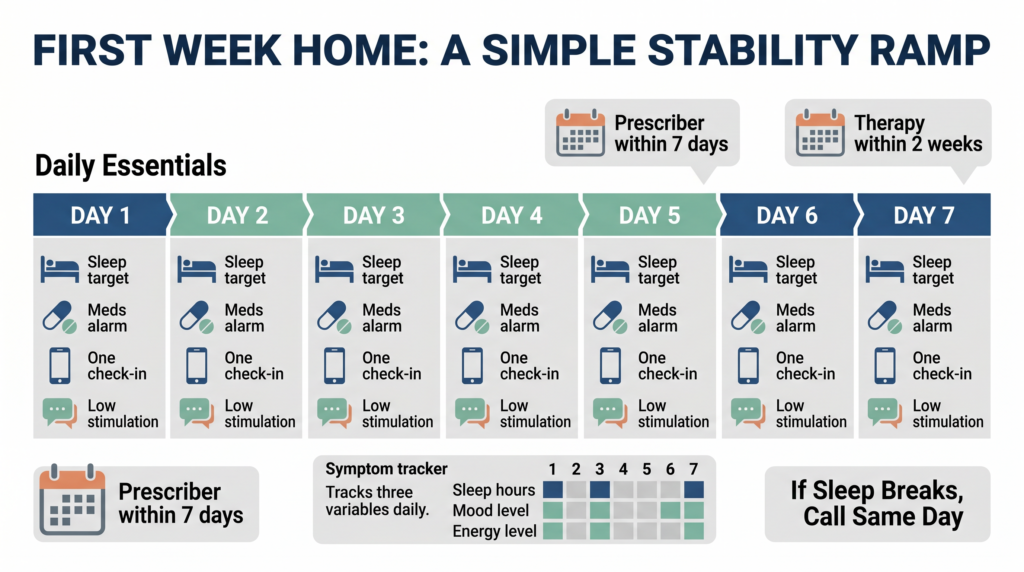
Sleep is the priority
For bipolar disorder, sleep disruption is not a minor issue—it’s a common pathway to relapse. Protect sleep immediately:
- Same wake time and bedtime every day
- Low stimulation evenings (dim lights, no heavy conflict, minimal scrolling)
- If sleep is breaking down, contact your prescriber—don’t “wait it out”
Medication on day one (no improvising)
- Take discharge meds exactly as prescribed starting the day you leave
- Use alarms and a pill organizer
- If you’re confused, call the unit, the pharmacy, or your outpatient clinic that day
Limit stimulation and demands
The first 2–3 days are not for catching up. Keep it simple:
- Minimal social obligations
- Minimal news/social media
- Basic food, hydration, shower, rest
- One supportive check-in per day is enough
The First Week at Home
Build a transition support system (daily contact)
- If possible, have someone stay with you—or check in daily
- If you live alone: set a daily “meds taken + sleep ok” text to a trusted person
- Consider peer support options for connection without over-explaining:
- NAMI programs: https://www.nami.org
- DBSA support groups: https://www.dbsalliance.org
Your prescriber follow-up is priority #1
Bring real data, not optimism:
- How many hours you slept each night
- Any emerging depression, agitation, racing thoughts, impulsivity, or suicidal thoughts
- Side effects and whether you’re tempted to stop meds
- Any substances used (honestly—this affects treatment decisions)
Therapy within the first 2 weeks
Early therapy goals:
- Process what happened (without judgment)
- Identify triggers/stressors that contributed
- Update relapse prevention
- Plan boundaries and pacing for work/social demands
Medication adherence: the critical variable
The post-discharge period is when people commonly stop meds because they feel improved, feel dulled, dislike side effects, or want control back. If you want to change anything, make it a prescriber conversation—not a solo decision.
Rebuilding Routine: The “Rhythm” Principle (IPSRT-aligned)
Even if you’re not formally doing IPSRT, the protective idea is the same: stability comes from predictable daily rhythms.
Start with five anchors:
- Consistent wake time
- Consistent bedtime
- Regular meals
- Daily social contact (low-demand counts)
- Consistent daily activity pattern (a simple walk, light chores, one errand)
Return to activities gradually (2–4 week ramp)
- Week 1: sleep + meds + food + hygiene + brief connection
- Week 2: add one small responsibility per day
- Weeks 3–4: phased return to work/school/social activities as tolerated
Processing the Hospitalization (Without Letting Shame Drive Recovery)
Common post-discharge emotions include relief, anger, grief, shame, and uncertainty. These feelings do not mean you’re “backsliding”—they mean you went through something intense.
Reintegration research frames discharge as the start of a longer adjustment process, not a clean reset.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC9140300/
What to do with shame
Say it directly in therapy:
- “I feel ashamed that I needed hospitalization.”
Shame becomes dangerous when it makes you hide symptoms next time. Hospitalization is a treatment intervention—not a character verdict.
Telling people what happened
You control disclosure.
- Work: “I had a medical issue that required hospitalization” is sufficient.
- Friends/family: share only what supports your recovery.
- Partner/family system: consider a few sessions of family/couples therapy to process impact and rebuild trust.
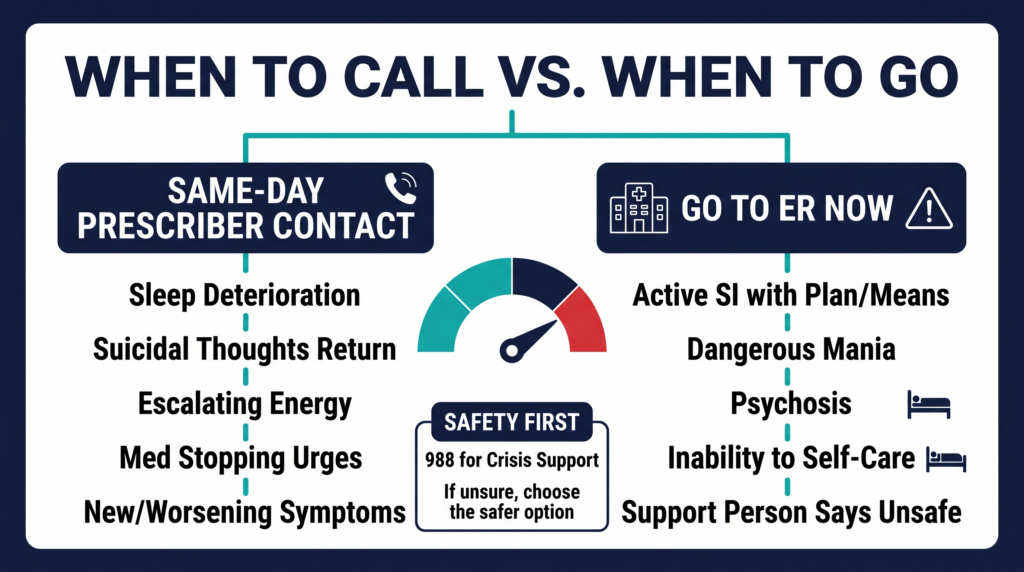
When Things Deteriorate After Discharge
Same-day contact with your prescriber if:
- Sleep is significantly worsening
- Suicidal thoughts return (even passive)
- Mood elevation, agitation, racing thoughts, escalating energy
- You stopped meds or strongly want to stop
- New/worsening symptoms that worry you
Return to the ER if:
- Active suicidal ideation with plan/means
- Severe mania with unsafe behavior you can’t interrupt
- Psychosis
- You cannot care for basic needs (food, hydration, safety)
- Your support person believes you are unsafe
Going back to the ER is not “failure.” It’s appropriate clinical decision-making when risk is rising faster than outpatient care can respond.
Resources for the Post-Hospitalization Period
- 988 (US): call/text for crisis support
- NAMI HelpLine: 1-800-950-6264 (resource navigation) — https://www.nami.org
- DBSA Support Groups: https://www.dbsalliance.org
- SAMHSA Treatment Locator: https://findtreatment.gov