
Bipolar Disorder And Suicide: Understanding The Risk And What To Do
If you live with bipolar disorder, or you love someone who does, you may already know this fear by name. You may have felt it at 2 a.m., when the room is quiet and your mind is not.
This topic matters because suicidal thoughts in bipolar disorder are common, dangerous, and treatable. You deserve clear facts, real warning signs, and a plan you can use when your brain starts lying to you.
If You Are In Crisis Right Now
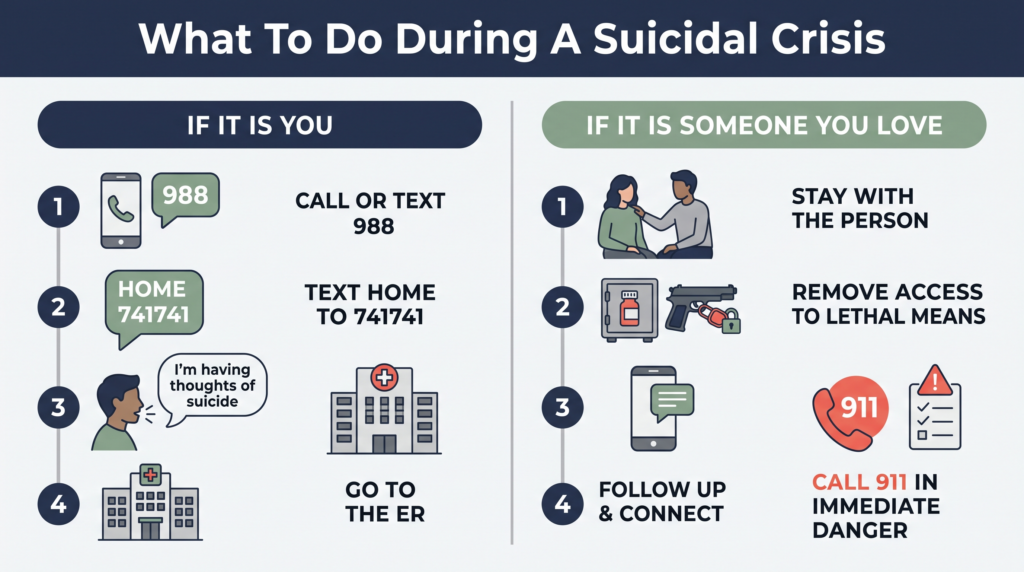
Call or text 988 for the Suicide & Crisis Lifeline. It is free, confidential, and open 24/7.
Text HOME to 741741 for the Crisis Text Line. You can also go to the nearest emergency room.
Call 911 if you or someone else is in immediate danger. You do not need to be certain you will act for this to count as an emergency.
This Is The Most Important Safety Topic On This Site
Bipolar disorder carries one of the highest suicide risks of any medical or psychiatric condition. That is a hard sentence to read, but I’d rather tell you the truth than leave you alone with guesswork.
Some recent analyses estimate that up to half of people with bipolar disorder attempt suicide at least once, and about 15% to 20% die by suicide. Other reviews place the annual suicide rate around 10 to 30 times higher than in the general population.
Some sources report even higher numbers, especially in older summaries and advocacy materials. The exact estimate varies by study, but the message does not: bipolar disorder suicide risk is very real.
These numbers are not here to scare you into despair. They are here because suicide is preventable, bipolar disorder is treatable, and hiding the danger never saved any of us.
At the individual level, treatment can sharply lower risk. Lithium, in particular, has some of the strongest evidence we have for reducing suicide in bipolar disorder.
Why Bipolar Disorder Carries Such High Suicide Risk
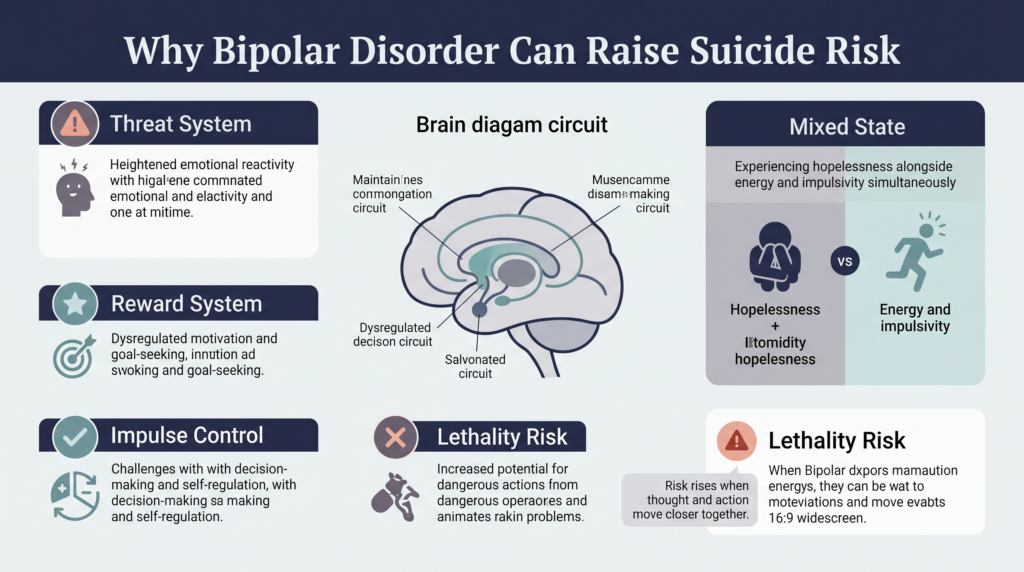
Your brain helps you judge threat, hope, reward, energy, and impulse control. Bipolar disorder can destabilize all of those systems at once.
That means the illness can shape both the pain of suicidal thinking and the speed of acting on it. You are not weak if this has happened to you. You are dealing with a condition that can hit the exact circuits that keep people alive.
The Biology Behind The Risk
When your brain’s threat system gets loud and your reward system goes dim, life can start to feel pointless and trapped. When the braking system for impulse control also weakens, the gap between thought and action can shrink.
That is part of why bipolar disorder can be so dangerous during certain mood states. It is not just sadness. It is sadness mixed with speed, agitation, urgency, and impaired judgment.
People with bipolar disorder also tend to use more lethal methods than the general population. This helps explain why the ratio of attempts to deaths is lower, and why every warning sign has to be taken seriously.
The Highest-Risk Mood States
Suicide risk in bipolar disorder is not spread out evenly across all moods. Some states are much more dangerous than others.
Mixed Episodes Are The Most Dangerous
A mixed episode is when depression and mania show up together. You feel hopeless, miserable, and flooded with pain, but you also have energy, agitation, and the ability to act.
That combination can be lethal. A person who feels dead inside but cannot move may stay stuck, while that same person with racing thoughts and restless energy may act fast.
If you are having suicidal thoughts during a mixed state, treat it like a psychiatric emergency. This is not a wait-and-see situation.
Depressive Episodes Carry Major Risk
Most suicidal deaths in bipolar disorder happen during depressive or mixed states, not classic euphoric mania. Bipolar depression can narrow your thinking until every door looks closed.
Hopelessness, shame, worthlessness, and the belief that nothing will change can make death seem like relief. If a depressive episode drags on without treatment response, the risk climbs.
The Transition Periods Can Be Dangerous
Coming out of depression can be risky too. The suicidal thinking may still be there even as your energy starts to return.
Rapid mood shifts can also raise danger. So can the days and weeks right after psychiatric hospital discharge, which research has repeatedly flagged as a high-risk period.
Who Is At Higher Risk Within The Bipolar Population
The strongest single predictor of a future suicide attempt is a past attempt. That does not mean another attempt is certain, but it does mean the risk deserves very serious attention.
Other factors that raise risk include family history of suicide, substance use, anxiety disorders, ADHD, and borderline personality disorder. Recent loss, unemployment, being socially isolated, and going long periods without treatment can also make things more dangerous.
Men are more likely to die by suicide, while women are more likely to attempt. Risk is also higher in people under 35 and in older adults, especially after major losses or medical decline.
Recent hospitalization matters too, especially in the first 30 days after discharge. If you or your loved one is in that window, tighter support is not overreacting. It is good safety practice.
The Role Of Treatment In Suicide Prevention
Treatment lowers suicide risk because it helps stabilize the brain systems that drive hopelessness, agitation, impulsivity, and extreme mood shifts. The evidence is strongest when care is consistent, not on-and-off.
If treatment has felt messy, disappointing, or exhausting, I get it. Still, untreated bipolar disorder is often far more dangerous than imperfect treatment.
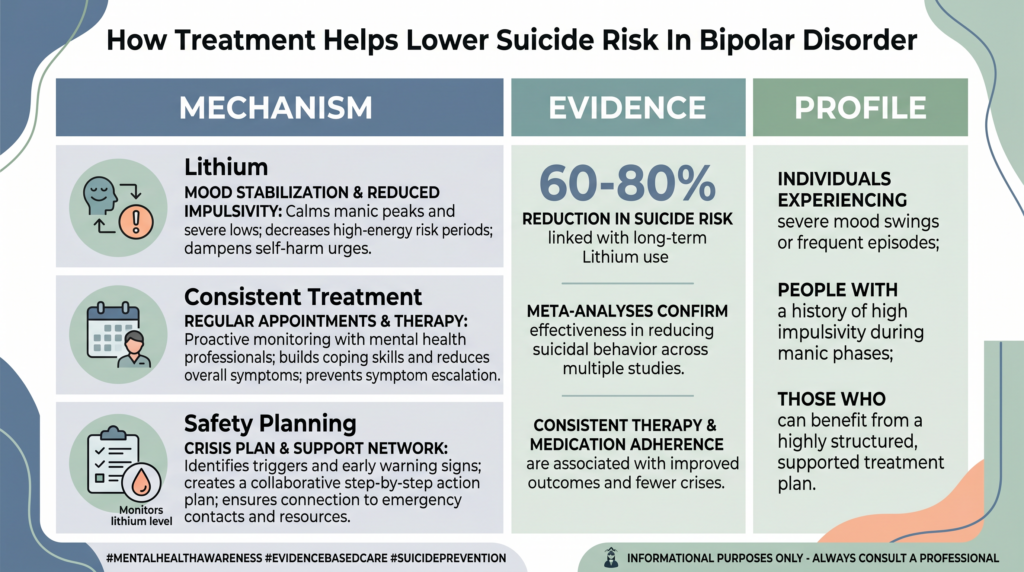
Lithium Has The Strongest Evidence
Mechanism: Lithium appears to steady the brain’s mood regulation systems and may reduce impulsivity and suicidal drive, partly through effects on serotonin and cell signaling. We do not understand every detail, but it seems to make the nervous system less chaotic and less likely to swing into dangerous states.
Evidence: Lithium has the clearest evidence of any bipolar medication for suicide prevention. Many studies and reviews show large reductions in suicide risk, often in the range of 60% to 80%.
Profile: Lithium tends to be most worth discussing if you have bipolar disorder with significant suicide risk, recurrent mood episodes, or past attempts. The key caveat is that it requires blood monitoring and can have side effects, so staying on it may take real support.
If you are not taking lithium and have never had a clear conversation with your prescriber about why, that conversation is worth having. It may not be right for you, but the topic should not be skipped.
Consistent Treatment Is The Foundation
Mechanism: Regular treatment reduces the intensity and frequency of mood episodes before they gather enough force to overwhelm judgment and hope. It also creates more chances for someone to notice warning signs early.
Evidence: People with bipolar disorder are more likely to die by suicide during periods of absent or inadequate treatment. That finding shows up again and again in the research.
Profile: This matters most for anyone who has had severe depression, mixed states, psychosis, past attempts, or recent hospitalization. The key caveat is that if side effects are pushing you away from treatment, the safer move is to tell your prescriber and adjust the plan, not quit care in silence.
Psychotherapy And Safety Planning Matter
Mechanism: Therapy can help you catch the thought traps that make suicide feel logical in the moment, and a safety plan gives your brain a script when it cannot think clearly. That lowers the odds that a temporary suicidal state turns into a fatal action.
Evidence: Safety planning is an evidence-based suicide prevention tool. CBT-based therapy also has evidence for reducing hopeless thinking and helping people respond more effectively to suicidal crises.
Profile: This helps almost everyone with bipolar disorder, but especially people with past suicidal thoughts, previous attempts, or unstable mood cycles. The key caveat is that a “no harm contract” is not enough, because it is not the same as a real safety plan.
Warning Signs In Yourself
Sometimes suicidal crisis looks loud. Sometimes it looks like quiet withdrawal and a strange calm.
Watch for passive thoughts like, “I wish I wasn’t here,” or “People would be better off without me.” Watch even more closely if thoughts become specific, such as thinking about how, when, or where you might die.
Other warning signs include giving away possessions, saying goodbye in a final-sounding way, isolating from people who care, or researching methods online. A sudden calm after severe distress can also be a red flag, because it may mean a decision has been made.
If any of this is happening, contact 988, your prescriber, or emergency services today. Not next week. Not at your next appointment.
Warning Signs In Someone You Love
Take any talk about death or wanting to die seriously. Direct statements matter, but indirect ones matter too.
Listen for things like, “There’s no point,” “I can’t do this anymore,” or “You won’t have to worry about me much longer.” Notice if they stop answering messages, pull away from everyone, give away meaningful things, or suddenly seem calm after days of intense distress.
Pay attention if they ask about access to medications, firearms, or other lethal means. If your gut says something is off, trust that signal and ask directly.
What To Do If You Are Having Suicidal Thoughts
First, make the situation smaller and safer. Put space between you and anything you could use to hurt yourself.
Call or text 988 right now. Text HOME to 741741, call someone you trust, or go to the nearest emergency room if you do not feel safe.
Then tell the truth plainly. Say, “I’m having thoughts of suicide.”
Do not soften it into “I’m struggling” or “I’ve been in a dark place” if what you mean is suicide. Your care team needs the clear version so they can respond to the real level of danger.
If you have medications, firearms, or other lethal means nearby, hand them to someone else, lock them away, or leave that location. This is not about punishment. It is about buying time until the wave passes.
Do not promise yourself you will keep this secret. Do not wait to see if it fades on its own.
And do not tell yourself that “just thoughts” do not count. Suicidal thoughts alone are enough reason to reach out.
What To Do If Someone You Love Is In Suicidal Crisis
Ask directly, “Are you thinking about suicide?” Research shows this does not plant the idea. It opens a door that may save a life.
If they say yes, stay with them. Call 988 together, or take them to the emergency room.
Do not leave them alone if you think the danger is immediate. If you have to step away to call for help, stay on the phone with them if you can.
Reduce access to lethal means right away. Store firearms with a trusted person if possible, use a lock, keep ammunition separate, and limit access to large amounts of medication.
This is not about distrust. It is about creating friction between a suicidal impulse and a fatal outcome.
Call 911 if the person is in immediate danger, refuses emergency help, or you believe their physical safety is at risk. If available, ask for a Crisis Intervention Team (CIT) officer.
After A Suicidal Crisis, The Risk Is Still High
Getting through one suicidal crisis does not mean the danger is gone. It means you survived this one, and now the next phase needs care too.
The first 30 days after psychiatric hospitalization are especially risky. Follow-up should happen fast, ideally within 7 days, and medications should continue without gaps.
If your discharge plan is vague, ask for specifics before you leave. If you are supporting someone else, this is the time to stay close, not step back because they seem “better.”
Tell someone what warning signs to watch for. Review what helped, what failed, and what needs to change in the safety plan.
Shame after a suicidal crisis is common. It also makes people hide the next one, so it needs to be talked about openly in therapy or with trusted support.
What A Safety Plan Should Include
A real safety plan is short, clear, and easy to use when your brain is overloaded. You do not want a document that reads like homework when you can barely breathe.
Include your personal warning signs first. Then list internal coping steps you can try, like moving to a safer room, taking a shower, grounding, or calling one specific person.
Next, list people you can contact and professionals you can contact. Add 988, your prescriber, your therapist, your local emergency room, and one trusted person who knows the plan.
Finally, write down how you will reduce access to lethal means. If you need help building this out, create one with your therapist, psychiatrist, or another clinician who understands suicide risk.
Resources You Can Use Today
- 988 Suicide & Crisis Lifeline: Call or text 988
- Crisis Text Line: Text HOME to 741741
- NAMI HelpLine: 1-800-950-6264 Monday through Friday, 10 a.m. to 10 p.m. ET
- AFSP: afsp.org
- DBSA: dbsalliance.org
- IASP International Crisis Centers: iasp.info/resources/Crisis_Centres
If you are outside the U.S., the IASP directory can help you find crisis support in your country. If you are in immediate danger anywhere, call your local emergency number now.
Charting Your Next Safe Step
If this post hits close to home, please do one small concrete thing before you close the page. Save 988 in your phone, text one safe person, or move one dangerous item out of reach.
You do not have to prove your pain is severe enough. If suicide is on the radar, that is enough to ask for help now.