How Bipolar Disorder Is Diagnosed: The Complete Evaluation Process
You’ve been tracking your moods for months now, and the pattern is undeniable. Three weeks of unstoppable energy where you reorganized your entire apartment at 3 a.m., followed by a crash so deep you couldn’t answer texts for two weeks.
Your doctor mentioned bipolar disorder, but you’re wondering: how is bipolar disorder diagnosed, and why does it take so long to get a clear answer?
The diagnostic process isn’t a single blood test or brain scan. It’s a methodical investigation that rules out dozens of other conditions, maps your mood history across months or years, and matches your experience against specific clinical criteria that distinguish bipolar disorder from depression, anxiety, ADHD, or borderline personality disorder.
Understanding how clinicians reach a bipolar diagnosis helps you become an active participant in your own evaluation. You’ll know what information matters most, which symptoms to track, and why your earliest warning signs hold more diagnostic weight than your current state.
Key Takeaways
- Medical causes must be ruled out first — thyroid disorders, vitamin deficiencies, and neurological conditions can mimic bipolar symptoms perfectly
- Your mood history over time is more important than your current symptoms — clinicians need to see the polarity pattern across multiple episodes
- The DSM-5 requires specific duration and severity thresholds — mania must last at least 7 days for Bipolar I, hypomania at least 4 days for Bipolar II
- Screening tools like the MDQ are starting points, not diagnoses — they flag potential bipolar patterns but can’t replace comprehensive clinical evaluation
- Misdiagnosis is common — up to 40% of people with bipolar disorder are initially diagnosed with unipolar depression because they seek help during depressive episodes
Why Diagnosing Bipolar Disorder Is Complicated
Bipolar disorder doesn’t show up on lab work. Your brain chemistry shifts in ways that current imaging technology can’t capture in a single snapshot, and the condition reveals itself through behavioral patterns that unfold over months or years rather than days.
The biggest diagnostic challenge is that most people seek help during depressive episodes, not manic or hypomanic ones. When your brain’s reward circuitry gets stuck holding down the accelerator during mania, you feel invincible, creative, and deeply productive.
You’re not calling a psychiatrist because you finally have the energy to launch that business idea or reconnect with everyone you’ve ever known.
You call when the crash comes. And when you’re sitting in that first appointment describing weeks of hopelessness, insomnia, and inability to function, you look identical to someone with unipolar depression. The clinician needs to excavate your mood history to find those earlier high periods you might not have recognized as symptoms.
Comorbidities muddy the picture further. Anxiety disorders, ADHD, substance use, and borderline personality disorder all share overlapping symptoms with bipolar disorder.
Racing thoughts could be anxiety, mania, or ADHD. Impulsivity could be hypomania or borderline traits. The right diagnosis requires teasing apart which symptoms cluster together during distinct mood episodes versus which ones persist regardless of your mood state.
Step 1 — Ruling Out Medical Causes
Before any psychiatrist applies a bipolar diagnosis, they need to confirm your mood instability isn’t caused by a physical condition that’s disrupting your nervous system regulation. Dozens of medical problems can create symptoms that look exactly like bipolar disorder.
Thyroid disorders are the most common mimics. When your thyroid produces too much hormone (hyperthyroidism), you experience racing thoughts, decreased need for sleep, irritability, rapid speech, and impulsive behavior that’s clinically indistinguishable from mania. When it produces too little (hypothyroidism), you get the fatigue, cognitive slowing, and depression that matches bipolar’s depressive pole.
Vitamin deficiencies — particularly B12, folate, and vitamin D — can destabilize mood dramatically. B12 deficiency causes depression, cognitive impairment, and irritability. Vitamin D deficiency correlates with both depressive and manic symptoms in people who already have bipolar disorder, making episodes more severe.
Neurological conditions like multiple sclerosis, epilepsy, brain tumors, and traumatic brain injury can all produce mood cycling. Temporal lobe epilepsy specifically can cause sudden mood shifts, irritability, and behavioral changes that mimic rapid-cycling bipolar disorder.
Medications and substances frequently trigger mood episodes. Corticosteroids (prednisone) can induce full manic episodes. Stimulants prescribed for ADHD can unmask underlying bipolar disorder. Antidepressants given for unipolar depression can flip someone with undiagnosed bipolar into mania, which is sometimes the first clue that the original diagnosis was wrong.
Your doctor will order blood work checking thyroid function (TSH, T3, T4), vitamin levels (B12, folate, vitamin D), complete blood count, metabolic panel, and potentially brain imaging if there’s any suggestion of neurological involvement. These tests don’t diagnose bipolar disorder, but they rule out conditions that would require completely different treatment protocols.

Step 2 — The Psychiatric Evaluation
Once medical causes are excluded, the diagnostic work shifts to mapping your mood patterns across time. This is where understanding bipolar disorder symptoms becomes critical, because you need to help your clinician see the full polarity pattern.
What It Involves
The psychiatric evaluation is a structured conversation, typically lasting 60-90 minutes for an initial assessment. Your clinician is building a timeline of your mood episodes, identifying triggers, and looking for the specific symptom clusters that define bipolar disorder versus other conditions.
You’ll discuss your current symptoms in detail, but the clinician will spend more time on your history. They want to know about every period in your life when your mood, energy, or behavior shifted significantly from your true baseline. They’re looking for discrete episodes with clear beginnings and endings, not just general moodiness.
What You Will Be Asked
Expect questions about manic or hypomanic episodes: Have you ever had a period lasting at least several days when you felt so good or hyper that others thought you weren’t your normal self? When you needed much less sleep than usual but didn’t feel tired? When you were much more talkative, your thoughts raced, or you couldn’t slow your mind down?
You’ll be asked about depressive episodes: Have you had periods of at least two weeks when you felt sad, empty, or hopeless most of the day, nearly every day? When you lost interest in almost everything? When your energy dropped so low that even small tasks felt impossible?
Sleep architecture gets particular attention because it’s one of the most reliable markers of mood state. Your clinician wants to know: During high periods, did you sleep less but still feel rested and energetic? During low periods, did you sleep excessively but still feel exhausted? Changes in sleep often precede mood shifts by days, making them your earliest warning sign.
Questions about impulsivity and risk-taking help distinguish hypomania from normal good moods. Did you spend money you didn’t have? Make major life decisions impulsively? Engage in sexual behavior that was out of character? Quit jobs or end relationships suddenly? These behaviors during elevated mood periods suggest the impaired judgment that defines mania rather than just feeling happy.
Family history matters significantly. Bipolar disorder has strong genetic components, with first-degree relatives of people with bipolar disorder having 5-10 times higher risk than the general population. If your parent or sibling has bipolar disorder, your clinician weighs that heavily in the diagnostic picture.
Why Your Mood History Is the Most Critical Factor
Current symptoms tell your clinician where you are right now. Mood history tells them what condition you have. Someone with unipolar depression and someone with bipolar depression can present identically in a depressive episode, but their treatment needs are completely different.
The polarity pattern is what distinguishes bipolar disorder. Your clinician needs to see that you’ve experienced both poles — elevated mood (mania or hypomania) and depressed mood — in distinct episodes separated by periods of relative stability or by direct switches from one pole to the other.
This is why keeping a mood tracking inventory before your evaluation is invaluable. If you can show your clinician a chart of your mood, sleep, and energy levels over the past three months, you’ve given them data that would otherwise take multiple appointments to extract through conversation. You can learn more about living with bipolar disorder and developing these tracking habits.
The challenge is that many people don’t recognize their hypomanic episodes as symptoms. You remember feeling productive, creative, and confident. You don’t remember that you also slept three hours a night, started five projects you never finished, and irritated everyone around you with rapid-fire speech. Your clinician needs to help you reframe those “good” periods as potential mood episodes.
Step 3 — Applying the DSM-5 Criteria
Once your clinician has mapped your mood history, they compare your experience against the standardized diagnostic criteria in the DSM-5. This is how they determine not just whether you have bipolar disorder, but which type.
What the DSM-5 Is
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) is the reference guide that mental health professionals in the United States use to diagnose psychiatric conditions. It provides specific criteria that must be met for each diagnosis, ensuring consistency across clinicians.
The DSM-5 doesn’t explain why you have bipolar disorder or how to treat it. It’s purely a classification system that says: if your symptoms match this pattern, this is the diagnosis. Think of it as a field guide for identifying mental health conditions based on observable symptoms and reported experiences.
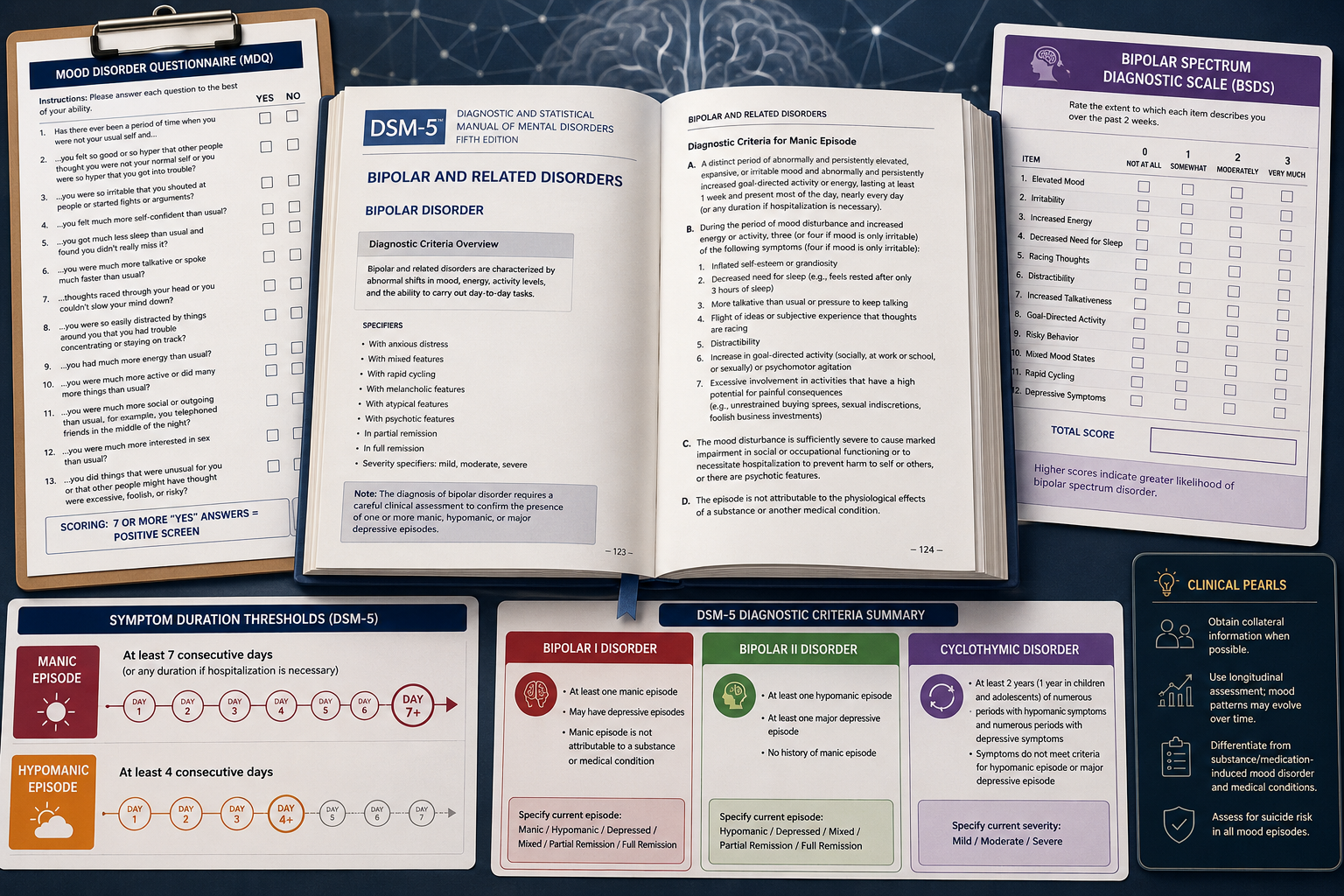
DSM-5 Criteria for Bipolar I Disorder
Bipolar I disorder requires at least one manic episode. That manic episode must meet all of these criteria:
A distinct period of abnormally and persistently elevated, expansive, or irritable mood and increased goal-directed activity or energy, lasting at least 7 consecutive days (or any duration if hospitalization is required), present most of the day, nearly every day.
During that period, at least three of these symptoms (four if the mood is only irritable):
- Inflated self-esteem or grandiosity
- Decreased need for sleep (feeling rested after only 3 hours)
- More talkative than usual or pressure to keep talking
- Flight of ideas or racing thoughts
- Distractibility
- Increase in goal-directed activity or psychomotor agitation
- Excessive involvement in risky activities
The episode must cause marked impairment in social or occupational functioning, require hospitalization to prevent harm, or include psychotic features. It can’t be attributable to substances or another medical condition.
You don’t need to have experienced a depressive episode to be diagnosed with Bipolar I, though most people with Bipolar I do experience both poles over time. The presence of even a single manic episode is sufficient for the diagnosis.
DSM-5 Criteria for Bipolar II Disorder
Bipolar II disorder requires at least one hypomanic episode and at least one major depressive episode. You cannot have ever had a full manic episode (if you have, the diagnosis is Bipolar I).
A hypomanic episode meets the same symptom criteria as mania but with key differences:
- Lasts at least 4 consecutive days (shorter than mania’s 7-day requirement)
- Represents a clear change from usual functioning that’s observable by others
- Does not cause marked impairment in functioning
- Does not require hospitalization
- Does not include psychotic features
A major depressive episode requires at least 5 of these symptoms during a 2-week period, representing a change from previous functioning, with at least one symptom being either depressed mood or loss of interest:
- Depressed mood most of the day, nearly every day
- Markedly diminished interest or pleasure in all or almost all activities
- Significant weight loss or gain, or change in appetite
- Insomnia or hypersomnia nearly every day
- Psychomotor agitation or retardation
- Fatigue or loss of energy
- Feelings of worthlessness or excessive guilt
- Diminished ability to think or concentrate
- Recurrent thoughts of death or suicidal ideation
The distinction between Bipolar I and II isn’t about severity. Bipolar II’s depressive episodes are often more frequent, longer-lasting, and more treatment-resistant than those in Bipolar I. The difference is in the upper pole: mania versus hypomania.
DSM-5 Criteria for Cyclothymic Disorder
Cyclothymic disorder is a milder but more chronic pattern of mood cycling. For at least 2 years (1 year in children and adolescents), you’ve experienced numerous periods of hypomanic symptoms (not meeting full criteria for a hypomanic episode) and numerous periods of depressive symptoms (not meeting full criteria for a major depressive episode).
During that 2-year period, the symptoms have been present for at least half the time, and you’ve never been without symptoms for more than 2 months at a time. You’ve never met criteria for a major depressive, manic, or hypomanic episode.
Cyclothymic disorder often develops into Bipolar I or II disorder over time. It represents a temperamental instability that may be a precursor to more severe mood episodes.
DSM-5 Changes From Earlier Versions
The DSM-5 made several important changes from the DSM-IV that affect how bipolar disorder is diagnosed:
Increased emphasis on energy and activity changes, not just mood. The criteria now require “increased goal-directed activity or energy” during manic and hypomanic episodes, recognizing that some people experience primarily activation changes rather than euphoria.
Mixed features specifier replaced the DSM-IV’s “mixed episode” diagnosis. Now you can have a manic, hypomanic, or depressive episode “with mixed features” if you have symptoms from the opposite pole during the episode. This better captures the reality that many people experience simultaneous symptoms from both poles.
Antidepressant-induced mania is no longer automatically excluded from counting toward a bipolar diagnosis. If manic symptoms persist beyond the physiological effect of the antidepressant, they can count as a manic episode, which helps identify people whose underlying bipolar disorder was unmasked by antidepressant treatment.
Step 4 — Screening Tools
Screening questionnaires can’t diagnose bipolar disorder, but they help identify people who should undergo comprehensive evaluation. Your clinician might use one or more of these tools as part of the diagnostic process.
The Mood Disorder Questionnaire (MDQ)
The Mood Disorder Questionnaire is a 13-item self-report screening tool that asks about lifetime history of manic or hypomanic symptoms. You answer yes or no to questions like “Has there ever been a period of time when you were not your usual self and you felt so good or so hyper that other people thought you were not your normal self?”
The MDQ also asks whether several symptoms happened during the same period and whether they caused significant problems. A positive screen requires yes answers to at least 7 of the 13 symptom questions, confirmation that several occurred together, and acknowledgment of moderate or serious problems.
The MDQ has good sensitivity (detecting true cases) but moderate specificity (ruling out non-cases). It’s useful for flagging potential bipolar disorder in people being treated for depression, but it generates false positives in people with borderline personality disorder or ADHD.
The Bipolar Spectrum Diagnostic Scale (BSDS)
The Bipolar Spectrum Diagnostic Scale presents a paragraph describing a person with bipolar disorder and asks you to rate how well it describes your own experience. It’s designed to capture the full bipolar spectrum, including subsyndromal presentations that don’t meet full DSM criteria.
The BSDS is particularly good at identifying Bipolar II disorder, which is often missed by tools focused on more severe manic symptoms. It has higher specificity than the MDQ, meaning fewer false positives, but may miss people with less typical presentations.
Limitations of Screening Tools
All screening tools share fundamental limitations. They rely on self-report, which means you need to recognize and accurately report your symptoms. Many people don’t identify their hypomanic periods as problematic, leading to false negatives.
Screening tools can’t distinguish bipolar disorder from conditions with overlapping symptoms. A positive screen might indicate bipolar disorder, borderline personality disorder, ADHD, or substance use disorders. They’re starting points for conversation, not diagnostic endpoints.
Cycle awareness before treatment selection is critical. A screening tool might suggest bipolar disorder, but your clinician still needs to map your specific polarity pattern, identify your earliest warning signs, and understand your trigger-and-response patterns before recommending treatment. You can’t match the intervention to your episode without understanding your unique cycling pattern.
Common Reasons for Misdiagnosis
Up to 40% of people with bipolar disorder are initially misdiagnosed, most commonly with unipolar depression. Understanding why misdiagnosis happens helps you advocate for accurate evaluation.
Seeking help during depression is the primary cause. When you’re in a depressive episode, you look identical to someone with major depressive disorder. If you don’t spontaneously mention past periods of elevated mood (and many people don’t, because they felt good during those times), your clinician has no reason to suspect bipolar disorder.
Hypomania is hard to recognize as a symptom. Unlike mania, which causes obvious impairment and often leads to hospitalization, hypomania can feel like your best self. You’re productive, social, creative, and confident. You might mention these periods to your therapist as “good weeks” without realizing they’re mood episodes that need to be factored into your diagnosis.
Comorbid conditions obscure the bipolar pattern. If you have ADHD, your baseline includes distractibility, impulsivity, and racing thoughts. When hypomania adds those same symptoms, the change might not be obvious. If you have anxiety, your baseline includes racing thoughts and agitation, which can mask hypomanic activation.
Substance use complicates the picture significantly. Stimulants can mimic mania. Alcohol and sedatives can mimic depression. If you’re using substances to self-medicate mood instability, your clinician needs to see your mood patterns during periods of sobriety to make an accurate diagnosis. Learn more about managing bipolar disorder and substance use.
The right med for the wrong cycle sometimes reveals the correct diagnosis. Many people are diagnosed with bipolar disorder only after antidepressants trigger a manic or hypomanic episode. The antidepressant didn’t cause bipolar disorder, it unmasked it by destabilizing a mood regulation system that was already vulnerable.
Borderline personality disorder shares many features with bipolar disorder: mood instability, impulsivity, relationship problems, and suicidal ideation. The key distinction is timing. Bipolar mood episodes last days to weeks and are often triggered by sleep disruption or seasonal changes.
Borderline mood shifts last hours to days and are typically triggered by interpersonal events. But distinguishing these patterns requires careful history-taking that doesn’t always happen in brief clinical encounters.
What Happens If You Think You’ve Been Misdiagnosed
If you’ve been treated for depression but the treatment isn’t working, or if antidepressants made you feel agitated, irritable, or “wired,” consider whether bipolar disorder might be a better explanation for your symptoms.
Bring data to your next appointment. Start tracking your mood, sleep, and energy levels daily for at least a month before you talk to your doctor. Use a simple 1-10 scale for mood (1 = severely depressed, 10 = extremely elevated) and note hours of sleep and subjective energy level. This gives your clinician objective data about your mood patterns.
Describe past “good” periods explicitly. Don’t wait for your doctor to ask about mania or hypomania. Volunteer information about times when you felt unusually energetic, needed less sleep, were more talkative or social than usual, started multiple projects, or engaged in impulsive behavior. Frame these as “I’m not sure if this is relevant, but…” and let your clinician assess.
Ask for a comprehensive re-evaluation. If you’ve only had brief medication management appointments, request a full diagnostic evaluation with a psychiatrist or psychologist who specializes in mood disorders. Bring any past psychiatric records, including medication trials and responses.
Consider a second opinion. If your current provider dismisses your concerns about misdiagnosis, you’re entitled to seek evaluation from another clinician. Bipolar disorder is complex enough that diagnostic disagreements between competent clinicians are common. A fresh perspective can be valuable.
Don’t stop medications without medical supervision. If you’re currently taking antidepressants and suspect you might have bipolar disorder, don’t stop them abruptly. Sudden discontinuation can cause withdrawal symptoms and mood destabilization. Discuss your concerns with your prescriber and make any medication changes under their guidance.
Understanding what happens after a bipolar diagnosis can help you prepare for the next steps if your diagnosis changes.
After the Diagnosis
Getting a bipolar diagnosis often brings relief mixed with grief. Relief because you finally have an explanation for years of confusing mood shifts. Grief because you’re facing a chronic condition that requires ongoing management.
Your diagnosis is a starting point, not a destination. The label “bipolar disorder” tells you which category of treatments to explore, but it doesn’t tell you which specific medications, therapy approaches, or lifestyle modifications will work for your nervous system. That discovery process takes time.
Expect a period of treatment adjustment. Finding the right medication protocol typically takes 3-6 months of careful trials. Your psychiatrist will likely start with a mood stabilizer like lithium, valproate, or lamotrigine, or an atypical antipsychotic like quetiapine. You’ll need to weigh the side-effect trade-off against symptom relief, and that calculation is personal. Learn about bipolar disorder medication options and their mechanisms.
Build your cycle awareness before fine-tuning treatment. The first few months after diagnosis are ideal for intensive mood tracking. You want to identify your polarity pattern: Do you cycle seasonally? Does sleep disruption trigger episodes? How long do your episodes typically last? What are your earliest warning signs? This self-knowledge lets you match interventions to your specific cycling pattern.
Protect your sleep architecture above everything else. Decades of clinical data show that sleep disruption is the most common trigger for both manic and depressive episodes. Consistent sleep and wake times, even on weekends, provide more mood stability than any single intervention except medication. This isn’t optional self-care, it’s primary prevention.
Consider therapy alongside medication. Cognitive-behavioral therapy adapted for bipolar disorder, interpersonal and social rhythm therapy, and family-focused therapy all show efficacy in reducing relapse rates and improving functioning. Therapy helps you develop the trigger-and-response awareness that lets you intervene early when episodes start. Explore talk therapy options for bipolar disorder.
Connect with others who understand. Bipolar disorder can feel isolating, especially when you’re learning to manage it. Support groups provide practical wisdom from people who’ve navigated the same challenges. They’ll tell you which side effects are worth tolerating and which ones to push back on, how to talk to employers about accommodations, and how to maintain relationships through mood episodes.
Educate your support system. The people closest to you need to understand what bipolar disorder is and isn’t. They need to know your earliest warning signs so they can alert you when you’re cycling into an episode. They need to understand that irritability during depression or grandiosity during hypomania aren’t character flaws, they’re symptoms. Consider sharing resources about how family and friends can help.
Sustainable stability is the goal. You’re not aiming for perfect mood flatness or the elimination of all emotional variation. You’re aiming for a life where mood episodes are less frequent, less severe, and less disruptive. Where you can work, maintain relationships, and pursue your goals without being derailed by your brain chemistry every few months.
The diagnostic process might feel frustratingly slow, but it’s laying the foundation for everything that comes next. Accurate diagnosis lets you access the right treatments, understand your patterns, and build a management protocol that works for your specific nervous system.
Frequently Asked Questions
Can bipolar disorder be diagnosed with a blood test or brain scan?
No. There’s no biological test that can diagnose bipolar disorder. The diagnosis is based entirely on your symptom history and pattern of mood episodes over time. Blood tests and brain scans are used only to rule out medical conditions that can mimic bipolar symptoms.
How long does it take to get a bipolar diagnosis?
It varies widely. Some people are diagnosed after a single manic episode that leads to hospitalization. Others spend years being treated for depression before a clinician recognizes the bipolar pattern. On average, people with bipolar disorder experience a 5-10 year delay between symptom onset and accurate diagnosis.
Can you have bipolar disorder without manic episodes?
If you’ve never had mania or hypomania, you don’t meet criteria for bipolar disorder. However, some people have their first hypomanic episode years after their first depressive episode, which is when the diagnosis changes from unipolar depression to bipolar disorder. This is why ongoing monitoring is important.
What’s the difference between bipolar disorder and borderline personality disorder?
Both involve mood instability, but the timing differs. Bipolar mood episodes last days to weeks and often have biological triggers (sleep disruption, seasonal changes). Borderline mood shifts last hours to days and typically have interpersonal triggers (perceived rejection, abandonment fears). Many people have both conditions.
Do I need to see a specialist to get diagnosed with bipolar disorder?
While primary care doctors can diagnose bipolar disorder, psychiatrists and psychologists specializing in mood disorders have more training in distinguishing bipolar from similar conditions. If your presentation is complex or you’ve been misdiagnosed before, a specialist evaluation is worth pursuing.
Will a bipolar diagnosis affect my job or insurance?
Mental health diagnoses are protected health information under HIPAA. Your employer cannot access your medical records without your permission. However, a diagnosis can affect life insurance and disability insurance applications. Discuss these concerns with your provider when considering formal diagnosis versus treatment without documentation.
Charting Your Next Baseline
The diagnostic process for bipolar disorder is methodical because it has to be. Your treatment, your prognosis, and your understanding of yourself all depend on getting the diagnosis right. A comprehensive evaluation that rules out medical causes, maps your mood history, applies standardized criteria, and uses screening tools appropriately gives you the foundation for everything that follows.
If you’re in the middle of this process right now, be patient with it. Bring your mood data, describe your full history including the “good” periods, and advocate for thorough evaluation. The time invested in accurate diagnosis saves years of ineffective treatment.
If you’ve just received a bipolar diagnosis, you’re standing at the beginning of a learning curve. You’ll discover your polarity pattern, identify your earliest warning signs, find the medication protocol that balances efficacy against tolerability, and build the lifestyle structure that protects your sleep architecture and nervous system regulation.
Sustainable stability is possible. It requires ongoing attention, treatment adherence, and cycle awareness, but thousands of people with bipolar disorder maintain careers, relationships, and meaningful lives. Your diagnosis is not a limitation, it’s information. Use it to build the management protocol that lets you live fully.