Just Diagnosed With Bipolar Disorder: What to Know and What to Do First
You’re not broken, and you didn’t fail. When you’ve just been diagnosed with bipolar disorder, that’s the first thing you need to hear, because the diagnosis itself can feel like proof that something fundamental went wrong.
It didn’t.
Your brain’s mood regulation system operates differently, and now you finally have a name for the patterns that have been disrupting your life. Between 1-2% of adults worldwide live with bipolar disorder, and decades of clinical data show that with the right management protocol, most people achieve sustainable stability and build lives they genuinely want to live.
The weeks after diagnosis feel like standing at the base of a mountain you didn’t choose to climb. You’re exhausted from the symptoms that brought you here, overwhelmed by medical terminology, and probably terrified about what this means for your future. That’s completely valid.
This article walks you through exactly what to do first, how to understand your specific condition, and how to build the foundation for long-term stability without the hype or the false promises.
Key Takeaways
- Your first 90 days focus on cycle awareness before treatment selection: understanding your polarity pattern and earliest warning signs matters more than rushing into medication decisions.
- Bipolar disorder requires matching the intervention to your episode type: lithium shows superior prophylactic efficacy for bipolar I with 81-month median relapse-free survival, while atypical antipsychotics like quetiapine work better for depressive phases.
- Medication adjustment takes 8-12 weeks minimum: you’ll need to navigate the side-effect trade-off while your psychiatrist finds the right med for the wrong cycle.
- Sleep architecture protection is non-negotiable: disrupted sleep triggers both manic and depressive episodes, making consistent sleep/wake times your most powerful behavioral intervention.
- Crisis planning starts on day one: identifying your trigger-and-response patterns and building your support system now prevents hospitalization later.
You Just Got a Diagnosis. Now What?
The diagnosis lands differently for everyone. Some people feel relief that their experiences finally have a name. Others feel anger, grief, or complete disbelief. You might cycle through all of these emotions in a single afternoon.
There’s no correct way to respond when a psychiatrist tells you that you have a chronic mental health condition that will require lifelong management.
Right now, you probably have a prescription in your hand or an appointment scheduled to discuss medication options. You might be Googling frantically, reading horror stories about side effects and wondering if you’ll ever feel normal again. Slow down. You don’t need to have everything figured out today.
The most important thing you can do in the first 72 hours is simply let the information settle. Your brain needs time to process this, and rushing into decisions while you’re in shock rarely leads to good outcomes.
The Emotional Stages of a Bipolar Diagnosis
Shock and Disbelief
Your first reaction might be “the doctor got it wrong.” Especially if you’ve been functioning relatively well between episodes, or if you’ve been misdiagnosed with unipolar depression for years, the bipolar label can feel like it came out of nowhere. You’ll replay conversations, question whether you exaggerated your symptoms, and wonder if this is all a terrible mistake.
That’s your nervous system trying to protect you from information that feels too big to hold. Give yourself permission to sit with the disbelief without immediately trying to fix it.
Grief
You’re mourning the future you thought you’d have. The one where you didn’t need to think about medication blood levels, where you could pull all-nighters without triggering an episode, where your mood was just your mood and not a symptom to track.
This grief is real and it deserves space. You’re also grieving the past, reinterpreting years of experiences through a new lens and realizing how much of your suffering could have been prevented with earlier intervention.
Anger
It’s infuriating that your brain works this way. It’s infuriating that you have to deal with this while other people coast through life without tracking their sleep or worrying about medication side effects.
You might be angry at doctors who missed the diagnosis earlier, at family members who dismissed your symptoms, or at yourself for not recognizing the patterns sooner. Channel that anger into learning everything you can about your condition instead of letting it turn inward.
Relief
For many people, especially those who’ve struggled for years without understanding why, the diagnosis brings profound relief. You weren’t lazy, dramatic, or weak. You have a neurobiological condition with established treatment protocols.
The chaos finally makes sense. This relief can coexist with all the harder emotions, and it often becomes the foundation for acceptance.
Acceptance
Acceptance doesn’t mean you’re happy about having bipolar disorder. It means you’ve stopped fighting the reality of it and started focusing your energy on management instead of denial.
You’ll probably move in and out of acceptance many times, especially during difficult episodes. That’s normal. Acceptance is a practice, not a destination.
What Bipolar Disorder Is — And Isn’t
Let’s cut through the confusion with plain English. Bipolar disorder is a condition where your brain’s mood regulation system gets stuck in extreme positions instead of staying in a functional middle range.
When your brain’s reward circuitry holds down the accelerator, you experience mania or hypomania: elevated mood, racing thoughts, decreased need for sleep, impulsive behavior, and a feeling of untouchable power.
When those same circuits slam on the brakes, you crash into depression: profound sadness, no energy, disrupted sleep, loss of interest in everything, and sometimes thoughts of suicide.
Understanding the difference between bipolar I and II matters because treatment approaches vary. Bipolar I involves full manic episodes that typically last at least a week and often require hospitalization.
Bipolar II features hypomania, which is less severe and doesn’t include psychotic features, paired with major depressive episodes that tend to be longer and more treatment-resistant. Both are serious conditions that require professional treatment.
Here’s what bipolar disorder isn’t: it’s not a personality flaw, it’s not caused by weak character, and it’s not something you can positive-think your way out of. It’s also not a death sentence for your goals, relationships, or quality of life. With proper treatment, most people with bipolar disorder achieve remission and maintain it for years at a time.

Your First Priorities After Diagnosis
1. Find or Confirm a Good Psychiatrist
If the doctor who diagnosed you isn’t a psychiatrist, you need to see one within the next two weeks. Bipolar disorder is too complex for general practitioners to manage alone.
A good psychiatrist will spend time understanding your specific episode history, ask detailed questions about your family psychiatric history, and explain treatment options without pushing a single approach. They should be willing to answer your questions about medication mechanisms and side effects in language you can understand.
Red flags include: rushing you through appointments, dismissing your concerns about side effects, or prescribing without explaining why they’re choosing a particular medication for your polarity pattern.
You’re allowed to get a second opinion. You’re allowed to switch doctors if the relationship isn’t working. Working with your doctor is a partnership, not a dictatorship.
2. Understand What Treatment Will Involve
Treatment for bipolar disorder typically combines medication with therapy and lifestyle modifications. The medication piece usually starts with a mood stabilizer like lithium or an atypical antipsychotic like quetiapine, depending on whether you’re currently in a manic, hypomanic, or depressive phase.
Lithium works by modulating intracellular signaling pathways that stabilize circadian rhythms and enhance neuroprotection. Clinical data shows median relapse-free survival of 81 months for lithium in bipolar I, compared to 36 months for valproate and 42 months for carbamazepine.
Quetiapine targets depressive episodes by antagonizing dopamine and serotonin receptors, with effect sizes of 0.54-0.61 on depression rating scales over 8 weeks. The catch: lithium requires regular blood monitoring for kidney and thyroid function, and quetiapine often causes sedation and weight gain. This is the side-effect trade-off you’ll navigate with your psychiatrist.
Therapy, particularly cognitive behavioral therapy or interpersonal and social rhythm therapy, helps you identify triggers, regulate your daily routines, and develop coping strategies for mood shifts. Psychotherapy helps treat bipolar disorder by giving you tools that medication alone can’t provide.
3. Learn About Your Specific Type
Your diagnosis should specify whether you have bipolar I, bipolar II, or another variant like rapid-cycling (four or more episodes per year). This distinction determines your treatment approach.
Bipolar I responds well to lithium for maintenance, with rehospitalization rates of 26% over 2.5 years compared to 62% for carbamazepine. Bipolar II often requires different strategies, with antidepressants showing 40-60% response rates when combined with mood stabilizers, though they carry a 25% risk of triggering hypomania.
Ask your psychiatrist to walk you through your episode history and help you identify your polarity pattern. Do you tend to cycle into mania first, or does depression dominate? How long do your episodes typically last? What are your earliest warning signs? This information guides every treatment decision moving forward.
4. Start Tracking Your Mood
Before you can manage bipolar disorder effectively, you need to understand your personal patterns. Start a mood tracking inventory today. Use a simple 1-10 scale for mood, energy, and sleep quality.
Note any triggers you can identify: stressful events, sleep disruption, seasonal changes, alcohol use, or skipped medications once you start treatment. Track for at least 90 days to establish your true baseline and identify your cycle patterns.
This isn’t busywork. Cycle awareness before treatment selection is the difference between finding the right intervention quickly and spending years on medications that don’t match your episode type. Dealing with bipolar disorder requires this level of self-knowledge.
5. Tell the Right People
You don’t owe anyone an explanation about your diagnosis, but you do need a support system. Choose 2-3 people who’ve proven themselves trustworthy and tell them what’s happening. Explain what bipolar disorder actually is (not the media stereotype), what kind of support you need, and what your earliest warning signs look like so they can help you catch episodes early.
Be strategic about who you tell at work. You’re not required to disclose a mental health condition to your employer, but if your symptoms have affected your performance or you need accommodations, it might be worth having that conversation with HR. Document everything in writing.

What to Expect in the First Months
Medication Adjustment Period
Finding the right medication at the right dose takes time. Most mood stabilizers and antipsychotics require 4-8 weeks to reach full effectiveness, and you’ll likely need dose adjustments based on your response and side effects. Some people find the right combination quickly. Others spend 6-12 months trying different options. This is frustrating and exhausting, but it’s also completely normal.
Common side effects of bipolar disorder medications include weight gain, sedation, tremor, and gastrointestinal issues. Report everything to your psychiatrist, but don’t stop taking medication without medical supervision. Abrupt discontinuation can trigger severe mood episodes.
If you’re prescribed lithium, you’ll need blood tests every few months to monitor levels and kidney function. If you’re on valproate, liver function tests are essential. These aren’t optional. Long-term side effects of lithium are manageable with proper monitoring, but only if you actually do the monitoring.
Building Your Care Team
Your psychiatrist is essential, but they’re not enough. You need a therapist who specializes in bipolar disorder or at least has significant experience with mood disorders. You might benefit from a psychiatric nurse practitioner for medication management between psychiatrist appointments. Some people add a nutritionist, a sleep specialist, or a peer support specialist to their team.
Insurance makes this complicated and expensive. Advocate for yourself. Ask about sliding scale fees, community mental health centers, and university training clinics that offer reduced-cost services. Bipolar disorder support resources exist, but you have to actively seek them out.
Lifestyle Changes That Start Now
Protect your sleep architecture above everything else. Set a consistent bedtime and wake time, even on weekends. Your circadian rhythm directly affects mood stability, and sleep disruption is the most common trigger for both manic and depressive episodes. If you’re having trouble sleeping, address it immediately with your psychiatrist rather than letting it spiral.
Limit alcohol and avoid recreational drugs entirely. Substances interfere with medication effectiveness and destabilize mood. Nicotine affects your bipolar disorder by disrupting sleep and interacting with psychiatric medications, so if you smoke, consider this a priority for your quit plan.
Build routine into your days. Eat meals at consistent times. Exercise regularly, but not to extremion, which can trigger mania. The goal is nervous system regulation through predictable patterns, not perfection.
Bipolar Disorder Is a Lifelong Condition — Here’s What That Really Means
You’ll be managing this for the rest of your life. That’s the hard truth. There’s no cure, no finish line where you get to stop thinking about mood stability. But lifelong management doesn’t mean constant crisis.
Most people with bipolar disorder spend the majority of their time in remission once they find effective treatment. You’ll have episodes, but they become less frequent, less severe, and shorter with proper management.
Sustainable stability is the goal, not the absence of all symptoms. You’ll still have bad days. You’ll still experience stress and sadness and frustration like everyone else. The difference is that you’ll learn to distinguish between normal human emotions and the beginning of an episode, and you’ll have tools to intervene early.
Living with bipolar disorder means accepting that some things will always require more effort for you than they do for other people. Sleep hygiene isn’t optional. Medication compliance isn’t negotiable. Stress management isn’t a luxury. These are the non-negotiables that keep you stable.
Building Your Support System
You can’t do this alone, and you shouldn’t have to. What family and friends should know includes your warning signs, your crisis plan, and how to support you without enabling destructive behavior during episodes. Have explicit conversations about what helps and what doesn’t.
Some people need space during depressive episodes. Others need gentle accountability to get out of bed. Your support people can’t read your mind.
Consider joining a bipolar support group, either in person or online. Talking to people who actually understand what you’re going through reduces isolation and provides practical strategies that only lived experience can teach. The power of bipolar support groups lies in shared knowledge and mutual validation.
Set boundaries with people who aren’t helpful. If someone dismisses your diagnosis, suggests you just need to try harder, or treats you like you’re fragile and broken, limit your contact with them. You need people who see you as a whole person managing a medical condition, not as a diagnosis walking around.
Warning Signs to Watch for in the First Year
Learn your earliest warning sign for both mania and depression. For mania, it might be decreased need for sleep, racing thoughts, increased goal-directed activity, or irritability. For depression, watch for loss of interest in activities, changes in appetite, difficulty concentrating, or withdrawal from social contact. The earlier you catch an episode, the easier it is to intervene.
Seasonal patterns are common in bipolar disorder. Many people experience depression in fall and winter, with hypomania or mania emerging in spring. Track your patterns across a full year so you can anticipate and prepare for high-risk periods.
Stress is a universal trigger, but your specific stressors matter. Major life changes, relationship conflicts, work pressure, and sleep disruption all increase episode risk. You can’t eliminate stress, but you can develop better coping mechanisms and know when to increase support.
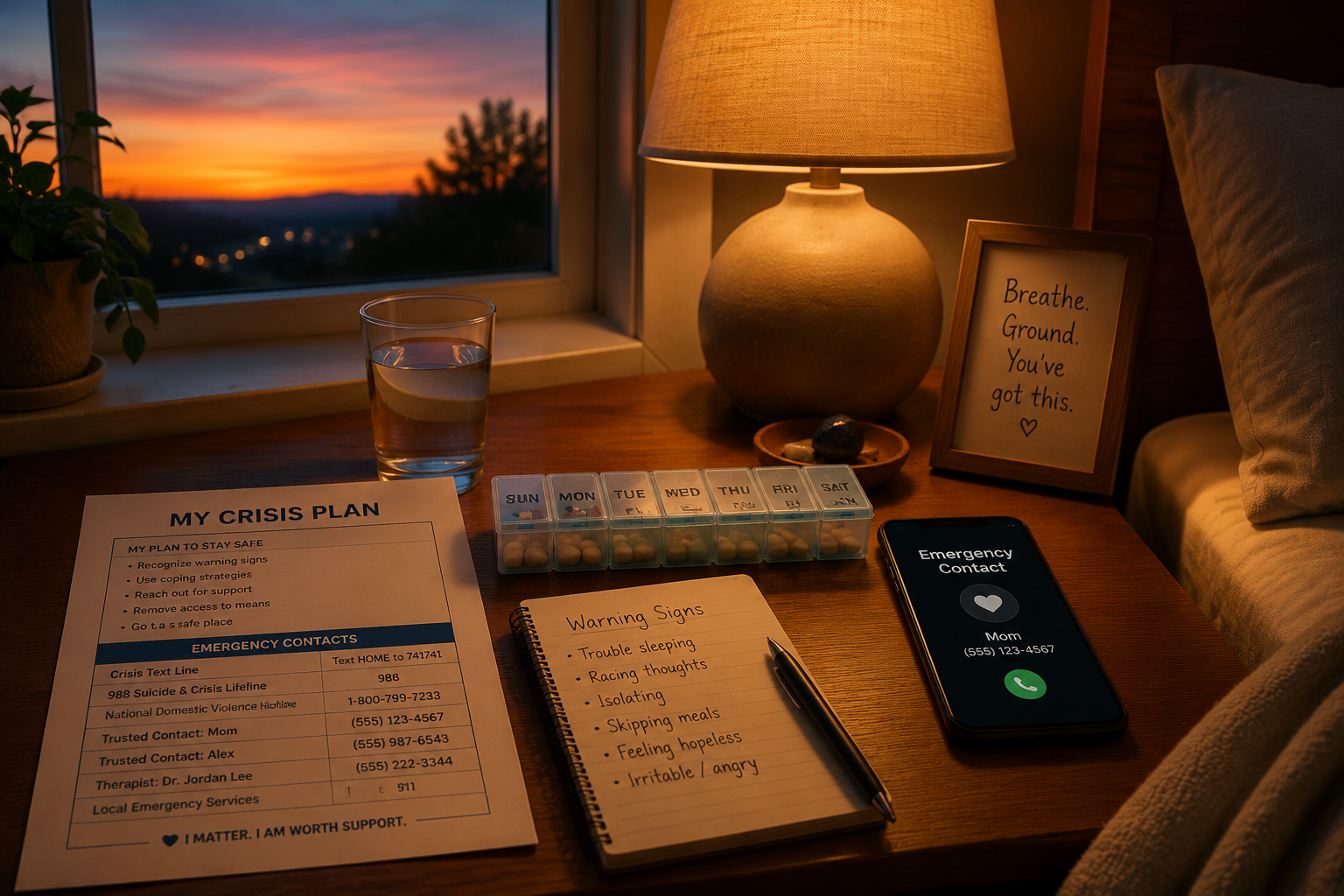
Crisis Planning From Day One
Hope for the best, but plan for the worst. Create a written crisis plan that includes: warning signs that you’re becoming unstable, names and phone numbers of your psychiatrist and therapist, trusted contacts who can help in an emergency, medications you’re taking, and instructions for when to go to the emergency room. Keep copies with your support people and in your phone.
Identify your crisis threshold. At what point do you need someone to take you to the hospital? What behaviors indicate you’re no longer safe to be alone? Having these conversations when you’re stable makes decision-making possible during a crisis when your judgment is impaired.
Remove access to means of self-harm during vulnerable periods. If you have suicidal thoughts during depressive episodes, don’t keep large quantities of medication at home. If you become reckless with money during mania, give a trusted person temporary control of your credit cards. These aren’t signs of weakness. They’re intelligent safety planning.
Charting Your Next Baseline
The first 90 days after diagnosis are about gathering information, not achieving perfection. You’re learning your patterns, adjusting to medication, building your support system, and figuring out what sustainable stability looks like for you specifically. This is hard work, and you’re doing it while managing symptoms that make everything harder.
You’ll make mistakes. You’ll miss doses, stay up too late, skip therapy appointments, and have moments where you want to quit the whole exhausting process. That’s part of the learning curve. What matters is that you keep showing up, keep tracking, keep communicating with your treatment team, and keep refining your management protocol based on what actually works for your brain.
Diagnosed with bipolar and wondering what’s next? The answer is: one day at a time, with increasing self-knowledge and decreasing fear. You’re building a life that accommodates your neurobiology instead of fighting against it. That’s not settling. That’s wisdom.
Your diagnosis doesn’t define you, but it does require your attention and respect. Give it both, and you’ll find your way to stability that lasts.
Frequently Asked Questions
How long does it take to feel stable after a bipolar diagnosis?
Most people need 3-6 months to find the right medication combination and dose, with full stabilization often taking 6-12 months. Your timeline depends on your episode severity, how quickly you respond to treatment, and how consistently you follow your management protocol.
Can I live a normal life with bipolar disorder?
Yes, though “normal” looks different for everyone. With effective treatment, most people with bipolar disorder maintain jobs, relationships, and pursue their goals. You’ll need to prioritize sleep, medication compliance, and stress management more than people without bipolar disorder, but sustainable stability is absolutely achievable.
Should I tell my employer about my bipolar diagnosis?
You’re not legally required to disclose a mental health condition unless it affects your ability to perform essential job functions. If you need accommodations or your symptoms have impacted your work, consider discussing it with HR and documenting everything in writing. Weigh the benefits of accommodations against potential stigma in your specific workplace.
What if the first medication doesn’t work?
It’s common to try multiple medications before finding the right match. Lithium works well for many people with bipolar I, but if you don’t respond or can’t tolerate the side effects, alternatives like valproate, carbamazepine, or atypical antipsychotics exist. Work closely with your psychiatrist and give each medication adequate time (usually 4-8 weeks) to assess effectiveness.
How do I know if I’m having a medication side effect or a new symptom?
Track everything in your mood journal with timestamps. New symptoms that start within days of a medication change or dose adjustment are likely side effects. Symptoms that develop gradually or match your historical episode patterns are more likely mood symptoms. When in doubt, contact your psychiatrist rather than guessing.
Is therapy really necessary if medication is working?
Yes. Medication stabilizes your brain chemistry, but therapy teaches you to recognize warning signs, manage triggers, regulate your daily routines, and develop coping strategies that medication alone can’t provide. The combination of medication and therapy consistently outperforms either treatment alone in long-term outcomes.