
Voluntary Psychiatric Hospitalization for Bipolar Disorder: What to Expect and How to Prepare
Sometimes you know you can’t keep doing this at home. Your brain is moving too fast, or sinking too low, or slipping too far from reality, and some part of you knows you need more help than a weekly appointment can give.
If that’s where you are, I want to say this first. Choosing voluntary psychiatric hospitalization for bipolar disorder is not giving up, and it is not proof that you failed.
Hospitalization As A Treatment Tool, Not A Failure
When bipolar symptoms get severe, your brain can stop managing danger in a reliable way. The circuits that help with judgment, sleep, impulse control, and reality testing can start misfiring hard enough that outpatient care is no longer enough.
That’s when hospitalization becomes a treatment tool. Not a punishment, not a character flaw, and not some permanent stain on your life.
For people with bipolar disorder, a hospital stay may be needed during severe mania with dangerous behavior, severe depression with active suicidal crisis, psychosis, or a medication crisis that needs 24-hour monitoring. It is a higher level of care for a higher-risk moment.
Voluntary hospitalization is also different from an involuntary hold. You are agreeing to treatment, which usually means more voice in decisions, more dignity in the process, and often less trauma.
A lot of people who admit themselves later say the same thing. They didn’t need more willpower, they needed containment, sleep, safety, and time for their brain to slow down enough to come back online.
When Voluntary Hospitalization Is The Right Choice
The best starting point is not fear. It’s self-knowledge.
You know the warning signs of your own mood shifts better than anyone else. You know what your early mania feels like, what your suicidal depression sounds like inside your head, and what it means when your usual coping tools suddenly stop working.
Clinical Indicators
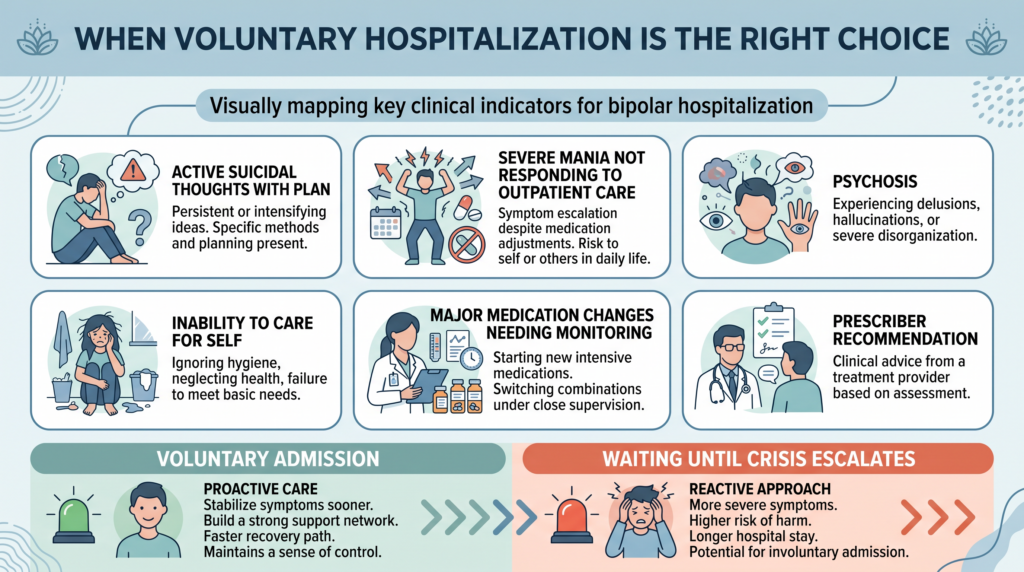
Voluntary hospitalization is often the right move when you are having active suicidal thoughts with a plan and you don’t trust yourself to stay safe outside the hospital. At that point, the issue is no longer whether you are “sick enough.” The issue is safety.
It can also make sense when a manic episode is escalating despite outpatient medication changes and you’re at risk of doing serious damage to your life, body, finances, or relationships. When your brain’s threat filter and brakes both go weak at once, bad outcomes can pile up fast.
Psychosis is another clear sign. If you are hearing voices, believing things that show you’ve lost contact with reality, or becoming too disorganized to function safely, you need a setting with close monitoring.
Hospitalization may also be the right choice if you are too depressed to care for yourself, or if medication changes need medical monitoring that can’t happen safely at home. If your prescriber tells you that you need the hospital, that recommendation usually comes from seeing risk that outpatient care can’t contain.
Choosing Voluntary Admission
If your psychiatrist recommends hospitalization and you agree, voluntary admission is usually the better path. You are entering treatment with more cooperation and usually more control over how information is shared and how decisions are discussed.
You can also go to a psychiatric ER yourself and ask for an evaluation for admission. That choice matters, because it shows insight, and insight often helps the whole process go more smoothly.
Voluntary status means you are not being held against your will at the start. It also means your participation in treatment decisions is usually stronger, though the team can still intervene if immediate safety becomes an issue.
How Voluntary Admission Works
A lot of fear comes from not knowing the sequence. The process feels less monstrous when you can see the steps.
Most voluntary admissions begin with evaluation, then paperwork, then intake, then transfer to the unit. The rhythm is rarely elegant, but that is usually the path.
The Admission Process
In many cases, admission starts in the psychiatric ER. You are evaluated, the team decides that hospitalization is appropriate, and if you agree, they begin the admission process.
Sometimes your outpatient psychiatrist can arrange a direct admission to a facility they work with. That route can bypass some ER chaos, but it depends on the hospital and bed availability.
You will usually sign consent forms for treatment. Read them if you can, ask questions if you need to, and remember that you have the right to understand what you are agreeing to.
Your rights should also be explained. If they aren’t, ask for them in writing.
What Happens During The Intake Evaluation
The intake evaluation is designed to answer a few urgent questions. What is happening now, how dangerous is it, what has already been tried, and what level of care do you need?
You will be asked about current symptoms, bipolar history, hospitalizations, medications, suicide risk, psychosis, substance use, sleep, and recent events. This is not the time to minimize.
Your medication list will be reviewed. In many hospitals, changes begin within the first 24 to 48 hours, especially if the episode is acute.
You will probably also get a medical assessment. That can include a physical exam, blood tests, and vital signs to rule out medical causes and make sure your body is stable enough for psychiatric treatment.
There will also be a safety screening of your belongings. That part can feel invasive, but the purpose is simple. They are removing anything that could be used for self-harm or accidental injury.
The Inpatient Environment
Psychiatric units are strange if you’ve never seen one before. They are more ordinary and more unsettling than most people expect.
You are still in a hospital. But it is a hospital built around safety, structure, and behavior, not privacy and comfort.
What The Unit Is Like
Most inpatient psychiatric units are locked. That is standard and does not mean you are a prisoner.
The locked door is there because people on the unit may be suicidal, psychotic, impulsive, confused, or unsafe to leave. The environment is controlled to reduce danger.
Some units are calm and quiet. Some are loud, understaffed, and full of tension.
That variation is real, and it can shape your experience a lot. You may have a private room or a roommate, depending on the facility.
You will have meals, nursing staff, access to doctors, and a schedule. You will also have less freedom than you have at home, because the hospital is trying to create predictability when your brain is not giving you much.
Daily Schedule
The daily rhythm is usually repetitive on purpose. Bipolar brains often do better when sleep, meals, light, and activity stop swinging around.
Mornings often start with vital signs, medication, and a nursing check-in. During the day, there may be one to three group sessions, meals, recreation, and brief contact with your psychiatrist or treatment team.
Those psychiatrist meetings are often shorter than people expect. Ten to twenty minutes a day is common.
Evenings usually include more medication, more vitals, and some kind of wind-down period. It can feel rigid, but that structure is part of the treatment.
What To Expect In Group Therapy
Groups usually focus on psychoeducation, coping skills, relapse prevention, and discharge planning. Some are useful, some are thin, and the quality depends a lot on the facility.
You do not have to share every detail of your life. In most groups, listening is allowed.
Also, the other patients will not all have bipolar disorder. Inpatient units are mixed, which can be comforting, awkward, or both.
Your Rights As A Voluntary Patient
The word “hospitalized” makes many people assume they lose all control. That is not how voluntary status usually works.
You still have rights, and it helps to know them before you need them. Clarity lowers panic.
Core Rights You Retain
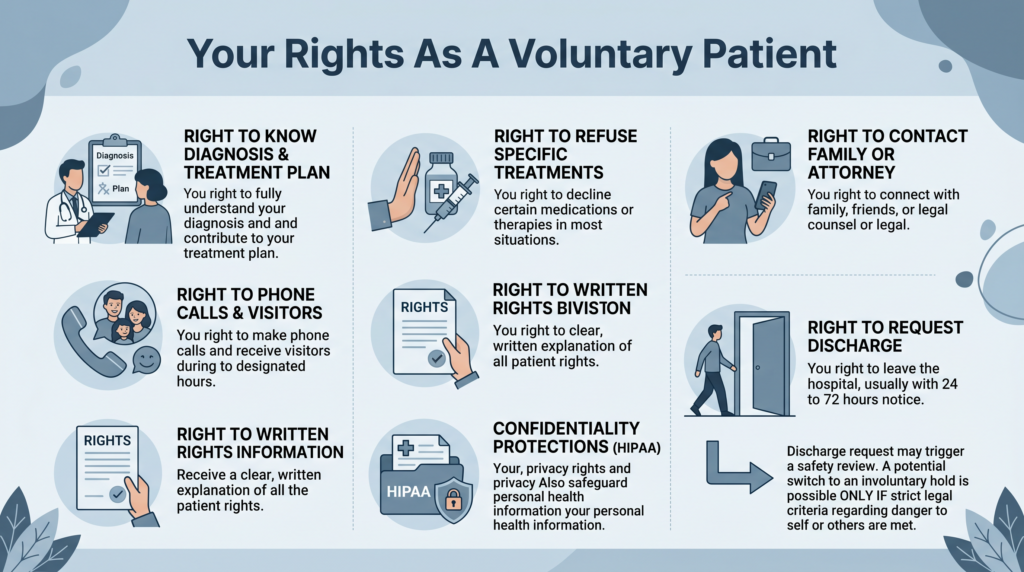
As a voluntary patient, you generally have the right to refuse specific treatments, unless there is an acute safety emergency. You also have the right to know your diagnosis, your treatment plan, and what medications are being recommended.
You can usually communicate with your family, support person, or attorney. Phone calls and visits are often limited to certain hours, but they are usually allowed.
You should also receive written information about your rights. Ask for it if no one offers it.
The Right To Discharge
One of the biggest differences with voluntary status is this. You can ask to leave.
That does not always mean you walk out that minute. Many facilities require notice, often 24 to 72 hours, so the team can assess safety and plan appropriately.
If you ask for discharge and the team believes you are still an immediate danger to yourself or others, they may try to convert your status to an involuntary hold. They cannot do that just because you are inconvenient. They need legal criteria.
Confidentiality
Your hospitalization is protected medical information. Staff should ask who they are allowed to speak with, and you get to control that list.
Your employer does not automatically get to know you were psychiatrically hospitalized. In most cases, you can simply say you had a medical hospitalization and leave it there.
What Gets Treated During Hospitalization
A psych unit is not designed to solve your whole life. It is designed to stabilize the part of your illness that has become dangerous.
That is important to understand going in. The goal is not total transformation. The goal is enough stability to get you safe and back into the right next layer of care.
Medication Stabilization
The main medical goal in inpatient bipolar treatment is often medication stabilization. When your mood circuitry is stuck on the accelerator, crushed under the floor, or breaking with reality, medication is often used to slow, lift, or reconnect those systems.
The evidence is strongest for using inpatient settings to start or adjust medications when symptoms are severe and close monitoring is needed. This setting tends to help most when mania, psychosis, suicidality, or major medication changes make outpatient trial-and-error unsafe.
In practice, that can mean starting or adjusting mood stabilizers, antipsychotics, or other medications while nurses watch for side effects and doctors track response day by day. Blood levels for medications like lithium or valproate can also be checked more quickly in the hospital.
Acute Safety
The second big goal is immediate safety. The unit removes access to means, adds observation, and creates enough friction that impulsive actions become harder.
Research and clinical practice both support this basic model. A secure environment with monitoring tends to help most when the immediate danger is self-harm, severe impulsivity, or rapidly escalating symptoms.
That means regular safety checks by staff, reduced access to dangerous objects, and intervention if your symptoms spike. It may not feel cozy, but it is built to keep you alive.
Stabilization Of Acute Episode
The third goal is to cool down the acute episode itself. For mania, that usually means reducing overstimulation, restoring sleep, and using medication to quiet the brain’s overfired reward and arousal systems.
For psychosis, treatment often focuses on antipsychotic medication, reorientation, and a lower-stimulation environment. For bipolar depression, the team may start or adjust treatment and watch closely, especially if suicide risk is high.
Preparing Practically For Hospitalization
If you know you are likely going in, practical prep helps. When your brain is flooded, small logistics can feel enormous.
Try to let a trusted person help. This is exactly the kind of moment support people are for.
What To Bring
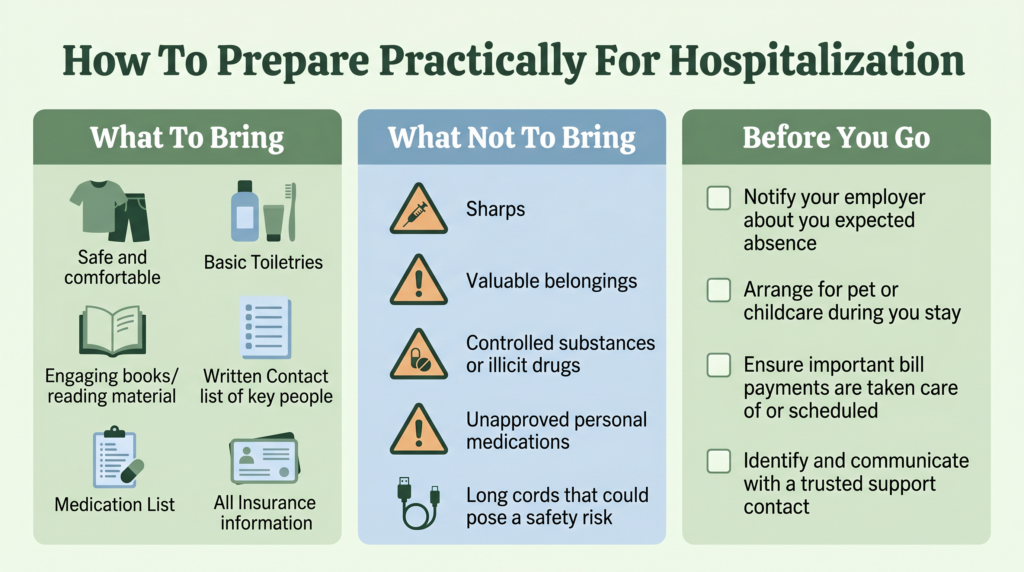
Bring comfortable clothes that meet the facility’s safety rules. Many units do not allow underwire bras, long drawstrings, metal-heavy clothing, or anything that could be used unsafely.
Bring simple toiletries in plastic packaging if the hospital allows them. Some places provide basics, but not all do.
Bring books, paper, or a coloring book if you want something to do without a phone. Bring a written list of phone numbers, because you may not have normal access to your contacts.
Also bring your medication list, insurance information, and ID if requested. If possible, leave originals and valuables at home and bring copies.
What Not To Bring
Do not bring razors, scissors, sharp objects, or anything the hospital has prohibited. Do not bring cash, jewelry, expensive electronics, substances, or your own medications unless they specifically tell you to.
Phone chargers are often restricted, especially long cords. Some facilities provide approved chargers and some do not, so call ahead if you can.
Practical Arrangements Before You Go
If work is an issue, you can keep it simple. “I have a medical situation that requires a brief hospital stay” is enough.
You do not owe your employer your psychiatric details. If you need job protection, FMLA may help if you qualify.
Try to set up pet care, childcare, plant care, bill payments, and anything else that would nag at you while you are there. Let one trusted support person know where you are going and how to reach the unit.
Length Of Stay: What To Expect
Most people imagine either one night or a month. In reality, it is usually somewhere in the middle.
Modern psychiatric hospital stays in the US are much shorter than they used to be. That is partly medicine, partly insurance, and partly system pressure.
Typical Duration
A typical acute inpatient stay for bipolar disorder is often around 5 to 14 days. The exact length depends on how severe the episode is, how quickly you respond to treatment, how safe discharge looks, and what your insurance approves.
Insurance matters more than most people expect. Continued stay reviews often require the hospital to prove that you still meet medical necessity criteria for each added day.
If you or your family think discharge is being pushed too early, speak up. Advocacy matters here.
Discharge Criteria
You are usually discharged when the acute safety crisis has eased, you have a place to go, outpatient follow-up is set, and your medication plan is clear enough to continue outside the hospital. It is not about being fully fixed.
Good discharge planning should start within the first 48 hours of admission. If no one has mentioned your next steps by then, ask.
Discharge Planning: The Most Important Part
The hospital stay gets the drama. Discharge planning does the real long-term work.
The days after discharge are fragile. Your brain may be better than it was, but not steady yet, and your old stressors will still be waiting at home.
What A Good Discharge Plan Includes
A solid discharge plan includes a psychiatric follow-up appointment within 7 days. Research consistently shows this lowers readmission risk and helps catch problems before they snowball.
It should also include a therapy appointment within 2 weeks, prescriptions ready before you leave, a crisis plan for the first few days at home, and clear contact information for what to do if symptoms get worse.
What To Ask Before You Leave
Ask direct questions. “What is my follow-up appointment, and is it confirmed?”
Ask, “Are my prescriptions ready?” Ask, “What should I do if I feel much worse before follow-up?”
Ask, “Who do I call if I have a medication question?” Ask, “What exactly changed in my treatment during this stay?”
The Post-Discharge Period: High Risk
The 30 days after psychiatric discharge are one of the highest-risk periods for relapse and suicide in bipolar disorder. Your environment comes rushing back in before your stability is fully rebuilt.
Research also shows that stopping meds after discharge raises readmission risk. One older but still cited study by Hassan and Lage, published in 2009, found a strong link between medication non-adherence and rehospitalization.
That does not mean discharge is doomed. It means this period deserves serious respect.
Charting Your Next Baseline
If you are considering voluntary psychiatric hospitalization for bipolar disorder, you are not weak. You are paying attention.
Sometimes the strongest thing you can do is admit that your brain needs more support than home can provide right now. Sometimes safety looks like handing the wheel to a treatment team for a few days so you can stop fighting your own mind alone.
If you choose to go in voluntarily, go in informed. Bring what you need, ask direct questions, protect your rights, and treat discharge planning like part of the treatment, not an afterthought.
And if you are reading this while deciding whether to go, trust what you already know. When your own warning signs are flashing red, listening to them is not surrender. It’s self-respect.