Bipolar Depression: Symptoms, How It Feels, and What Makes It Different
Sixty-nine percent of people with bipolar disorder are initially misdiagnosed. More than a third wait over a decade for an accurate diagnosis, and the most common wrong label they receive is major depression.
That’s not a failure of effort—it’s the nature of bipolar depression itself, which typically brings people to treatment long before mania ever does. You show up exhausted, heavy, unable to function, and hypomania feels too good to mention.
Bipolar depression isn’t just “the down part” of bipolar disorder. It carries its own distinct fingerprint, different from unipolar major depression in ways that matter enormously for treatment.
The medications that help stabilize bipolar depression aren’t always the same ones that work for major depression, and using the wrong intervention for the wrong cycle can make things worse. This is why cycle awareness before treatment selection isn’t just helpful—it’s essential.
Key Takeaways
- Bipolar depression feels qualitatively different from major depression: heavier, duller, with more hypersomnia and psychomotor slowing rather than agitation.
- Misdiagnosis is the norm, not the exception—most people with bipolar disorder initially receive a major depression diagnosis because they seek help during depressive episodes.
- Antidepressants alone carry significant risk of triggering mania or rapid cycling; mood stabilizers form the foundation of treatment.
- Suicide risk is higher in bipolar depression than in unipolar depression, making accurate diagnosis and appropriate treatment urgent.
- Treatment requires matching the intervention to your episode type—what works for mania won’t necessarily work for depression, and vice versa.
What Is Bipolar Depression?
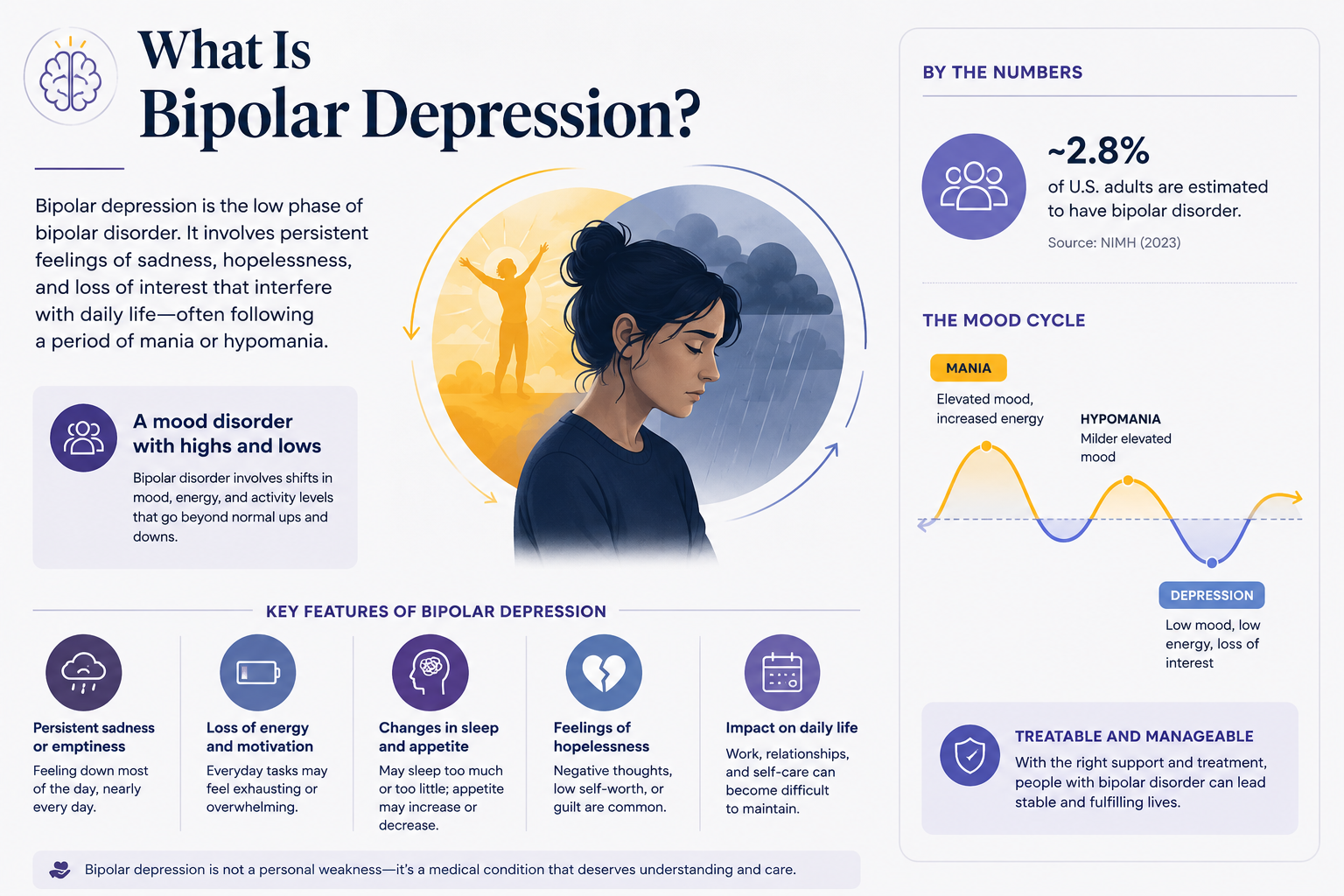
Bipolar depression is the depressive phase of bipolar disorder, a chronic condition marked by alternating episodes of depression, mania or hypomania, and sometimes mixed states. It’s not a separate diagnosis—it’s one polarity pattern within the larger bipolar spectrum.
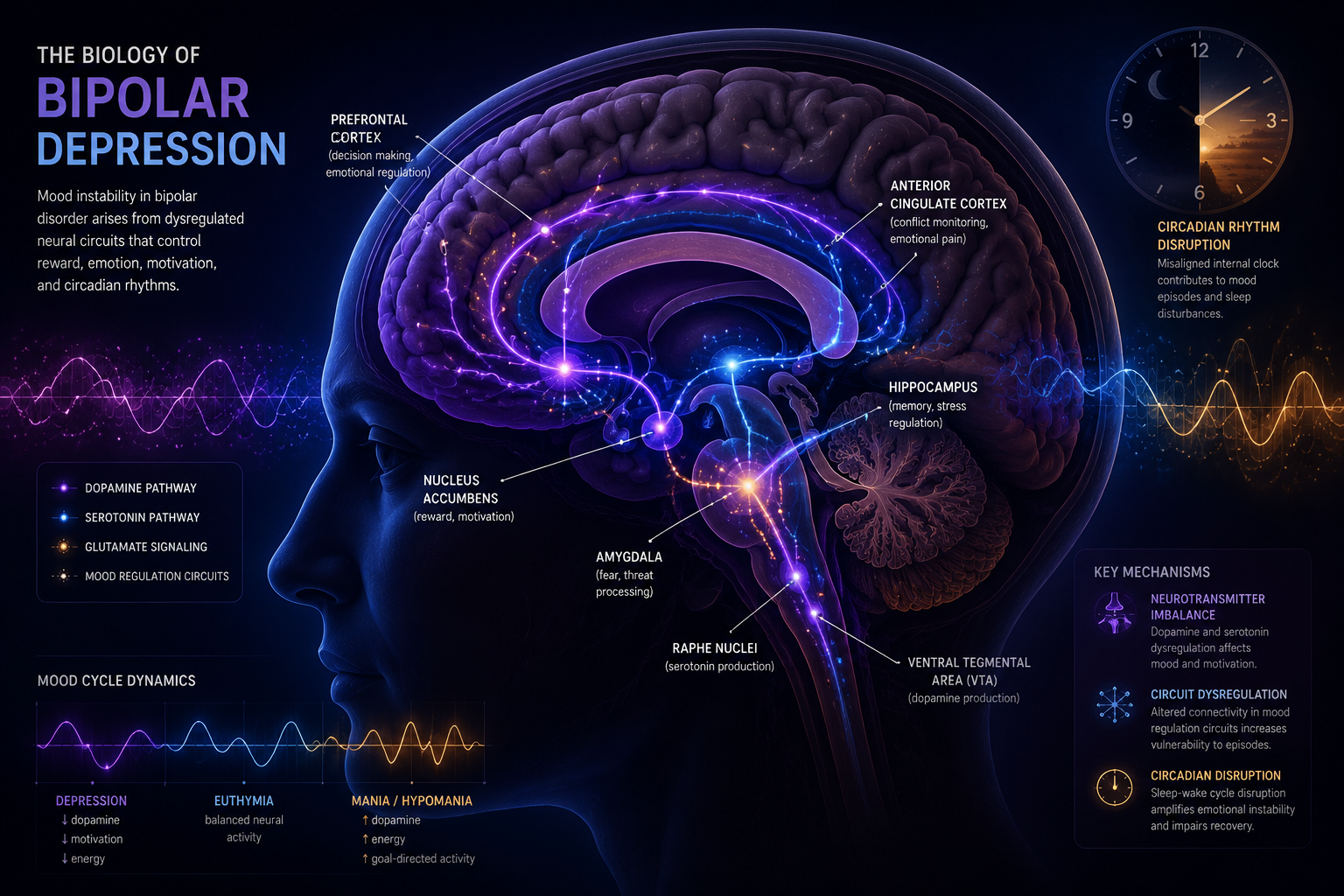
When your brain’s reward circuitry gets stuck holding down the brake instead of the accelerator, you experience the constellation of symptoms we call a depressive episode.
The biology involves multiple neurotransmitter systems. Dopamine pathways that normally drive motivation and pleasure become underactive. Serotonin regulation falters, affecting mood stability and sleep architecture.
The hypothalamic-pituitary-adrenal axis, your body’s stress response system, often shows dysregulation. Circadian rhythm disruption is nearly universal—your internal clock loses its anchor, making sleep patterns erratic and worsening every other symptom.
Bipolar depression occurs in both bipolar I and bipolar II disorder. In bipolar I, you’ve had at least one full manic episode—the kind that might land you in a hospital or cause serious life disruption.
In bipolar II, you experience hypomania (a milder, shorter elevated state) plus major depressive episodes. Both types spend far more time in depression than in elevated states, which is why understanding depressive episodes becomes the most urgent clinical task.
Episodes typically last two to three months on average, shorter than unipolar depression but with higher recurrence rates. You might cycle through multiple depressive episodes per year, especially if you have rapid-cycling bipolar disorder (four or more mood episodes annually). The pattern matters because it shapes your management protocol and helps predict your earliest warning signs.
How Bipolar Depression Feels: Inside a Depressive Episode
The subjective experience of bipolar depression has a particular quality that people describe as “heavy” or “dull” rather than simply sad. It’s not the sharp ache of grief or the anxious rumination of unipolar depression. It’s more like your entire nervous system has been wrapped in wet wool—everything slows down, dulls out, becomes effortful.
Hypersomnia is common, not insomnia. You might sleep ten, twelve, fourteen hours and still wake up exhausted. Your body feels weighted to the bed. Getting up to shower becomes a multi-hour negotiation with yourself. This is psychomotor retardation in plain English—your thoughts move like cold honey, your speech slows, your movements require conscious effort.
The anhedonia is profound. Activities that used to bring pleasure don’t just feel less enjoyable—they feel pointless, unreachable, as if they exist behind thick glass. You can’t imagine ever feeling differently. This isn’t pessimism you can talk yourself out of; it’s a neurobiological state where your brain’s reward prediction system has gone offline.
Concentration fractures. You read the same paragraph five times without retaining a word. Work tasks that used to take twenty minutes now take three hours, if you can complete them at all. Decision-making becomes paralyzing—even choosing what to eat feels overwhelming because your prefrontal cortex, responsible for executive function, is running on fumes.
Psychotic features appear more often in bipolar depression than in unipolar depression. You might develop delusions of guilt, poverty, or illness. Auditory hallucinations sometimes emerge. These aren’t “quirks”—they’re medical emergencies requiring immediate intervention, and they significantly elevate suicide risk.
The suicide risk in bipolar depression exceeds that of major depression. Decades of clinical data show that people with bipolar disorder attempt suicide at higher rates, and the lethality of attempts is greater. The combination of profound hopelessness, impaired judgment, and the impulsivity that can linger even during depression creates dangerous conditions.
Bipolar Depression vs. Major Depressive Disorder (Unipolar Depression)
What They Have in Common
Both conditions share the core diagnostic criteria for a major depressive episode: persistent low mood or loss of interest lasting at least two weeks, plus additional symptoms like changes in appetite, sleep disturbance, fatigue, feelings of worthlessness, concentration problems, and suicidal thoughts.
The DSM-5 criteria don’t distinguish between them during the depressive episode itself—the symptoms overlap almost completely.
Both cause significant functional impairment. You can’t work effectively, maintain relationships, or handle daily responsibilities. Both carry elevated suicide risk compared to the general population. Both respond to some degree to psychotherapy, particularly cognitive-behavioral approaches and interpersonal therapy.
The neurobiological substrates overlap too. Both involve monoamine neurotransmitter dysregulation (serotonin, norepinephrine, dopamine), HPA axis abnormalities, and inflammatory markers. Brain imaging shows similar patterns of reduced activity in prefrontal regions responsible for mood regulation.
The Key Differences
The phenomenology differs in subtle but consistent ways. Bipolar depression more often presents with hypersomnia rather than insomnia, though both can occur. Psychomotor retardation (that heavy, slowed-down feeling) is more characteristic of bipolar depression, while agitation and anxiety are more typical of unipolar depression.
The mood quality itself differs. People with bipolar depression describe their mood as “leaden” or “dull,” while those with unipolar depression more often report sadness, tearfulness, or anxious distress. Bipolar depression episodes tend to be shorter (two to three months average) but recur more frequently. Unipolar episodes often last longer (six months or more) with less frequent recurrence.
Psychotic features occur in roughly 10-15% of bipolar depression cases but only 3-5% of unipolar depression. When psychosis appears, it’s a strong signal toward bipolar diagnosis, though not definitive.
The treatment response pattern is the most clinically significant difference. Antidepressants alone can destabilize bipolar depression, triggering manic switches or rapid cycling. The odds ratio for manic switch with antidepressant monotherapy is 2.3—more than double the baseline risk. In unipolar depression, antidepressants are first-line treatment without this concern.
Mood stabilizers like lithium and lamotrigine, which form the foundation of bipolar disorder treatment, have limited efficacy in unipolar depression. Conversely, some interventions effective for unipolar depression (like certain antidepressants as monotherapy) actively harm people with bipolar depression.
Why This Distinction Is So Hard to Make
The diagnostic challenge is structural. Most people with bipolar disorder seek treatment during depression, not mania. Hypomania often feels good—increased energy, confidence, productivity, creativity. You don’t complain about feeling great. You might not even recognize it as abnormal, especially if episodes are brief or you’ve never experienced a contrasting depressive state.
When you finally see a clinician, you’re depressed. You describe low mood, sleep problems, concentration difficulties, suicidal thoughts. Without a clear history of mania or hypomania, the clinician has no reason to suspect bipolar disorder. They diagnose major depression and prescribe an antidepressant, which is the right med for the wrong cycle.
Family history helps but isn’t always available or accurate. Many people don’t know their relatives’ psychiatric histories. Stigma keeps diagnoses hidden. Even when family history is positive for bipolar disorder, it doesn’t guarantee the same diagnosis in you—it just raises the probability.
The retrospective identification of hypomania is unreliable. When you’re currently depressed, remembering past periods of elevated mood is difficult. Your brain’s state-dependent memory makes those times feel distant or unreal. Clinicians must ask specific questions about sleep need, goal-directed activity, risk-taking, pressured speech, and racing thoughts during “good” periods, not just “Have you ever felt too happy?”
Comorbidities muddy the picture further. ADHD, anxiety disorders, substance use, and personality features can all mimic or mask bipolar symptoms. A young adult with ADHD, social anxiety, and cannabis use who presents with depression creates a diagnostic puzzle that takes time and careful longitudinal observation to solve.
The Risk of Misdiagnosis
Misdiagnosis isn’t rare—it’s typical. Sixty-nine percent of people with bipolar disorder receive an incorrect initial diagnosis, most commonly major depression. One-third wait more than ten years for accurate diagnosis. During that decade, they often receive treatments that don’t work or actively worsen their condition.
The consequences are serious. Antidepressant monotherapy in unrecognized bipolar depression can trigger manic episodes, sometimes the first full manic episode a person experiences. This is called an antidepressant-induced switch, and it can be severe—requiring hospitalization, causing psychosis, damaging relationships and careers.
Even without frank mania, antidepressants alone can induce rapid cycling, where you experience four or more mood episodes per year. Once rapid cycling starts, it’s harder to stabilize. Your polarity pattern becomes more chaotic, and treatment becomes more complex.
The delay in appropriate treatment means years of unnecessary suffering. Mood stabilizers and atypical antipsychotics that could have provided relief go untried. Psychotherapy approaches specific to bipolar disorder, like interpersonal and social rhythm therapy, aren’t implemented. Your quality of life, relationships, and career all take hits that might have been preventable.
The misdiagnosis also affects your self-understanding. You might blame yourself for “treatment-resistant depression” when the real issue is that you’re being treated for the wrong condition. You might internalize a narrative of personal failure when the failure is diagnostic, not yours.
Depressive Episodes and Suicide Risk
Suicide risk in bipolar depression is substantially elevated compared to both the general population and unipolar depression. Approximately 25-50% of people with bipolar disorder attempt suicide at least once in their lifetime. Completed suicide rates are 10-20 times higher than in the general population.
The risk factors are multiple and interactive. The profound hopelessness and anhedonia of the depressive state create the desire to die. Impaired judgment and problem-solving make suicide seem like the only solution. Impulsivity, which can persist even during depression in people with bipolar disorder, increases the likelihood of acting on suicidal thoughts.
Mixed episodes—where depressive and manic symptoms occur simultaneously—carry the highest suicide risk. You have the despair of depression plus the energy and impulsivity of mania, a lethal combination. Agitation, racing thoughts, and severe insomnia during depression all elevate risk.
Psychotic features dramatically increase danger. Delusions of guilt (“I’ve ruined everything and everyone would be better off without me”) or command hallucinations (“You should kill yourself”) can directly drive suicidal behavior. These require immediate psychiatric intervention, often inpatient hospitalization.
Substance use, which is common in bipolar disorder, compounds risk. Alcohol and drugs impair judgment further, increase impulsivity, and worsen mood instability. The combination of bipolar depression and active substance use is a medical emergency.
If you’re experiencing suicidal thoughts, this is your earliest warning sign that your current management protocol isn’t sufficient. Contact your psychiatrist immediately. Call a crisis line (988 in the US). Go to an emergency room. This isn’t weakness or overreaction—it’s appropriate medical response to a life-threatening symptom.

Managing Bipolar Depression
Medication Approaches
Mood stabilizers form the foundation. Lithium has decades of clinical data supporting its efficacy in bipolar depression, though its effect size is modest. It works by modulating intracellular signaling pathways, enhancing neuroplasticity, and stabilizing circadian rhythms.
The median relapse-free survival on lithium reaches 81 months compared to 36 months for valproate and 42 months for carbamazepine. Lithium requires regular blood monitoring for levels, kidney function, and thyroid function—that’s the side-effect trade-off for its prophylactic benefits.
Lamotrigine shows particular efficacy for bipolar depression. It modulates glutamate release and stabilizes neuronal membranes. Clinical trials demonstrate significant improvement in depressive symptoms, with 56% of people at 200mg daily showing greater than 50% improvement versus 29% on placebo. Lamotrigine doesn’t typically trigger mania and is generally well-tolerated, though it requires slow titration to minimize rash risk.
Atypical antipsychotics, particularly quetiapine and lurasidone, have strong evidence for bipolar depression. Quetiapine works through multiple mechanisms—dopamine and serotonin receptor antagonism, norepinephrine reuptake inhibition via its metabolite. Multiple RCTs show significant MADRS score reductions starting at week one, with effect sizes of 0.54-0.61. The 2018 CANMAT/ISBD guidelines list it as first-line for both bipolar I and II depression.
Lurasidone demonstrates efficacy both as monotherapy and adjunctive to lithium or valproate. Six-week trials show significant depressive symptom reduction with good tolerability. It tends to be weight-neutral, addressing one of the major concerns with atypical antipsychotics.
Antidepressants remain controversial. When combined with a mood stabilizer, SSRIs show switch rates similar to mood stabilizer alone (15-27%), suggesting relative safety in that context. However, monotherapy carries substantial risk—odds ratio of 2.3 for manic switch. TCAs carry higher switch risk (around 10%) than SSRIs (around 3%). The evidence for antidepressant efficacy in bipolar depression is moderate at best, with response rates of 40-60% in acute phases.
The clinical approach is to start with a mood stabilizer or atypical antipsychotic, assess response over 4-6 weeks, and consider adding an antidepressant only if depression persists despite adequate mood stabilization. This is match the intervention to your episode in practice—you protect against mania while treating depression.
For more detail on medication options and their mechanisms, see our complete guide to bipolar disorder medications. Understanding common side effects helps you make informed decisions about the side-effect trade-off.
Therapy That Helps
Psychotherapy is essential, not optional. Medication addresses the neurobiological substrate, but therapy teaches you the skills to recognize patterns, manage triggers, and maintain stability.
Cognitive-behavioral therapy (CBT) helps you identify and modify the thought patterns that worsen depression. You learn to recognize cognitive distortions—catastrophizing, all-or-nothing thinking, personalization—and develop more balanced perspectives. CBT for bipolar disorder includes specific modules on medication adherence, sleep hygiene, and early warning sign recognition.
Interpersonal and social rhythm therapy (IPSRT) specifically targets the circadian and social rhythm disruptions central to bipolar disorder. You track your daily routines—sleep/wake times, meals, social interactions, physical activity—and work to stabilize them. The evidence shows that rhythm regularity reduces episode frequency and severity. This is protect your sleep architecture translated into structured intervention.
Family-focused therapy involves your close family members or partners in treatment. They learn about bipolar disorder, recognize warning signs, improve communication, and develop problem-solving skills. This matters because your support system’s understanding directly affects your stability and their own wellbeing.
Psychoeducation—learning about your condition, its mechanisms, treatment options, and self-management strategies—is itself therapeutic. Knowledge reduces fear, improves treatment adherence, and enables you to be an active participant in your care rather than a passive recipient. For more on therapeutic approaches, explore our guide to talk therapy for bipolar disorder.
Lifestyle Factors That Make a Difference
Sleep is non-negotiable. Disrupted sleep both triggers and perpetuates mood episodes. You need consistent sleep and wake times, even on weekends. Your bedroom should be dark, cool, and quiet.
Screens go off an hour before bed. Caffeine stops by early afternoon. If you’re struggling with sleep despite good habits, talk to your doctor—this might require medication adjustment.
Exercise has moderate antidepressant effects through multiple mechanisms: increased endorphin release, improved neuroplasticity, reduced inflammation, better sleep quality. You don’t need intense workouts—30 minutes of moderate activity most days provides benefit.
Walking, swimming, cycling, yoga all work. The key is consistency and finding something sustainable, not punishing yourself with exercise you hate.
Nutrition matters more than most people realize. Omega-3 fatty acids (from fish or supplements) have modest mood-stabilizing effects. Mediterranean-style diets rich in vegetables, whole grains, lean proteins, and healthy fats correlate with better mental health outcomes. Limiting alcohol is crucial—it disrupts sleep, destabilizes mood, and interacts with medications.
Stress management isn’t about eliminating stress (impossible) but developing nervous system regulation skills. Mindfulness meditation, progressive muscle relaxation, deep breathing exercises, and yoga all help downregulate your stress response. Even five minutes daily provides cumulative benefit.
Social connection protects against depression. Isolation worsens it. You need regular contact with supportive people, even when (especially when) you don’t feel like it. This might mean scheduling weekly calls with friends, attending a support group, or joining a class or club. For more on building your support network, see our resources on bipolar support groups.
Substance use requires honest assessment. Alcohol, cannabis, stimulants, and other drugs all destabilize mood and interfere with treatment. If you’re using substances to cope with symptoms, that’s a sign your treatment plan needs adjustment, not that you need more substances.
When to Talk to a Doctor
You should talk to a doctor if you’re experiencing depressive symptoms lasting more than two weeks, especially if they’re interfering with work, relationships, or daily functioning. Don’t wait until you’re in crisis—early intervention prevents episodes from deepening and reduces long-term impact.
Seek immediate help if you’re having suicidal thoughts, especially if you have a plan or means. This is a medical emergency, not something to “wait out.” Call 988 (Suicide and Crisis Lifeline), go to an emergency room, or call 911.
If you’ve been diagnosed with major depression but treatment isn’t working, or if antidepressants make you feel agitated, irritable, or “wired,” discuss bipolar disorder with your doctor. Bring up any history of periods where you needed less sleep, felt unusually energetic or confident, took risks you normally wouldn’t, or had racing thoughts.
If you have a family history of bipolar disorder, mention this to any mental health provider. It significantly increases your risk and should inform diagnostic consideration and treatment planning.
When choosing a provider, look for someone with specific experience in mood disorders. Psychiatrists have the most training in medication management. Psychologists, licensed clinical social workers, and licensed professional counselors can provide therapy. Ideally, you’ll have both a prescriber and a therapist, though they may be the same person.
Prepare for appointments by tracking your symptoms. Note mood patterns, sleep duration and quality, energy levels, concentration, and any concerning thoughts or behaviors. This mood tracking inventory becomes invaluable for accurate diagnosis and treatment monitoring. For guidance on working effectively with your treatment team, see our article on working with your doctor.
Charting Your Next Baseline
Bipolar depression isn’t just “feeling sad.” It’s a distinct neurobiological state with its own symptom profile, treatment requirements, and risks. The heaviness, the hypersomnia, the psychomotor slowing, the elevated suicide risk—these aren’t character flaws or personal failures. They’re medical symptoms of a treatable condition.
The path to sustainable stability starts with accurate diagnosis. If you’re reading this and recognizing yourself, that recognition is valuable data. Bring it to a qualified clinician. Describe not just your current depression but any past periods of elevated mood, reduced sleep need, increased activity, or impulsivity.
Treatment works, but it requires the right intervention matched to your specific polarity pattern. Mood stabilizers or atypical antipsychotics form the foundation. Antidepressants, if used at all, come only after mood stabilization and with careful monitoring.
Therapy teaches you the skills to recognize your earliest warning signs and maintain rhythm stability. Lifestyle factors—sleep, exercise, nutrition, stress management, social connection—aren’t optional extras but essential components of your management protocol.
Your true baseline isn’t the depression you’re experiencing now. It’s the stable, functional state that appropriate treatment can help you reach and maintain. Getting there requires patience, persistence, and partnership with knowledgeable providers. It requires self-knowledge—understanding your unique trigger-and-response patterns, your personal warning signs, your specific medication responses.
The decades of clinical data are clear: people with bipolar disorder can achieve long periods of stability, maintain relationships and careers, and live full lives. The median relapse-free survival on lithium is 81 months—nearly seven years. That’s not a ceiling; many people do even better. But it requires accurate diagnosis, appropriate treatment, and active self-management.
You’re not broken. Your nervous system is dysregulated in specific, understandable ways. The tools to address that dysregulation exist. Your job now is to access them, learn to use them, and build the sustainable stability you deserve.
Frequently Asked Questions
How long do bipolar depressive episodes typically last?
Bipolar depressive episodes average two to three months, shorter than unipolar depression episodes but with higher recurrence rates. Some people experience longer episodes, and rapid-cycling bipolar disorder involves four or more episodes per year. Episode duration varies individually and can be influenced by treatment adherence and lifestyle factors.
Can you have bipolar depression without ever experiencing mania?
Yes, in bipolar II disorder. You experience major depressive episodes and hypomania (a milder elevated state) but never full mania. Hypomania often feels good and may go unrecognized, which is why many people with bipolar II are initially misdiagnosed with major depression. Careful history-taking about past “good” periods is essential for accurate diagnosis.
Why can’t I just take antidepressants for bipolar depression?
Antidepressants without a mood stabilizer carry significant risk of triggering manic episodes or rapid cycling in bipolar disorder—the odds ratio for manic switch is 2.3. Even when combined with mood stabilizers, antidepressants show only moderate efficacy for bipolar depression. Mood stabilizers and atypical antipsychotics have better evidence and safety profiles as first-line treatments.
Is bipolar depression more dangerous than regular depression?
Suicide risk is substantially higher in bipolar depression than in unipolar depression. Approximately 25-50% of people with bipolar disorder attempt suicide at least once, and completed suicide rates are 10-20 times higher than the general population. The combination of profound hopelessness, impaired judgment, and impulsivity creates particularly dangerous conditions requiring careful monitoring and treatment.
How can I tell if my depression is bipolar or unipolar?
Look for past periods of elevated mood, reduced sleep need (not insomnia but needing less sleep), increased energy, racing thoughts, impulsivity, or risk-taking. Bipolar depression more often involves hypersomnia, psychomotor slowing, and a “heavy” or “dull” mood quality. Family history of bipolar disorder is also significant. Only a qualified clinician can make the diagnosis, but recognizing these patterns helps you provide relevant information.
What should I do if I think I’ve been misdiagnosed?
Schedule an appointment with a psychiatrist or mental health provider experienced in mood disorders. Bring documentation of your symptom history, including any periods of elevated mood, energy, or reduced sleep need. Describe your response to past treatments, especially if antidepressants made you feel agitated or “wired.” Request a comprehensive evaluation specifically considering bipolar disorder. Getting a second opinion is always reasonable when diagnosis is uncertain.