
Involuntary Psychiatric Holds: Your Rights And What Family Members Need To Know
When your brain is running hot, fear gets loud fast. If bipolar symptoms have ever pushed you or someone you love toward a crisis, you need facts that calm the room, name the danger clearly, and protect your rights.
This is one of those subjects people whisper about until they need it tonight. I want to walk you through involuntary psychiatric hold bipolar disorder basics in plain English, because panic makes everything harder and mystery makes it worse.
What An Involuntary Psychiatric Hold Is And Isn’t
An involuntary psychiatric hold is a legal way to keep someone in a psychiatric setting for emergency evaluation and short-term care, even if they say no. The goal is safety and stabilization during an acute mental health crisis.
It is not a punishment. It is not the same as an arrest, and it is not meant to be permanent.
In plain English, this usually comes up when a person seems likely to seriously hurt themselves, seriously hurt someone else, or cannot meet basic needs because their mind is too unwell. With bipolar disorder, that can happen during severe mania, psychosis, or a crushing depressive episode.
The Legal Definition
States use different words, but the core idea is similar. A qualified professional, and often a police officer, can start a hold if the legal standard is met.
That standard is usually about immediate danger or severe inability to care for yourself because of a mental health condition. It is not supposed to be used just because someone has bipolar disorder, is acting odd, or has made people uncomfortable.
The Most Common Standard: 5150 And Its Equivalents
You have probably heard the term 5150. That is California law, but people often use it as shorthand for any involuntary psychiatric hold.
Every state has its own rules, names, and timelines. A common first hold is up to 72 hours, but some states use shorter or longer periods.
During that window, the hospital or crisis unit evaluates the person and starts acute treatment if needed. Sometimes the person leaves before the full period ends because the team decides the legal criteria are no longer met.
The Three Legal Criteria For A Psychiatric Hold
Most states use some version of three core standards. The exact wording changes, but the structure stays pretty familiar.
1. Danger To Self
This means an immediate and serious risk of self-harm. The key word is immediate.
Examples include active suicidal thoughts with a plan and access to the method, a recent high-lethality attempt, or a clear statement of intent to die soon. A history of bipolar disorder, past attempts, or a vague statement like “I can’t do this anymore” may be deeply concerning, but by itself it often does not meet the legal standard.
2. Danger To Others
This means an immediate and serious risk of physical harm to another person. The threat usually needs to be specific, credible, and close in time.
Examples include saying you are going to hurt a particular person and having the means to do it, or acting violently during manic psychosis. General anger, shouting, or irritability usually is not enough on its own.
3. Gravely Disabled
This means a person cannot provide for basic needs like food, clothing, or shelter because of a mental health condition. This standard often matters in severe bipolar episodes where judgment has collapsed.
You might see this in mania when someone has not slept in days, is wandering, not eating, spending wildly, and cannot protect themselves. You might also see it in severe depression when a person is no longer able to manage basic self-care.
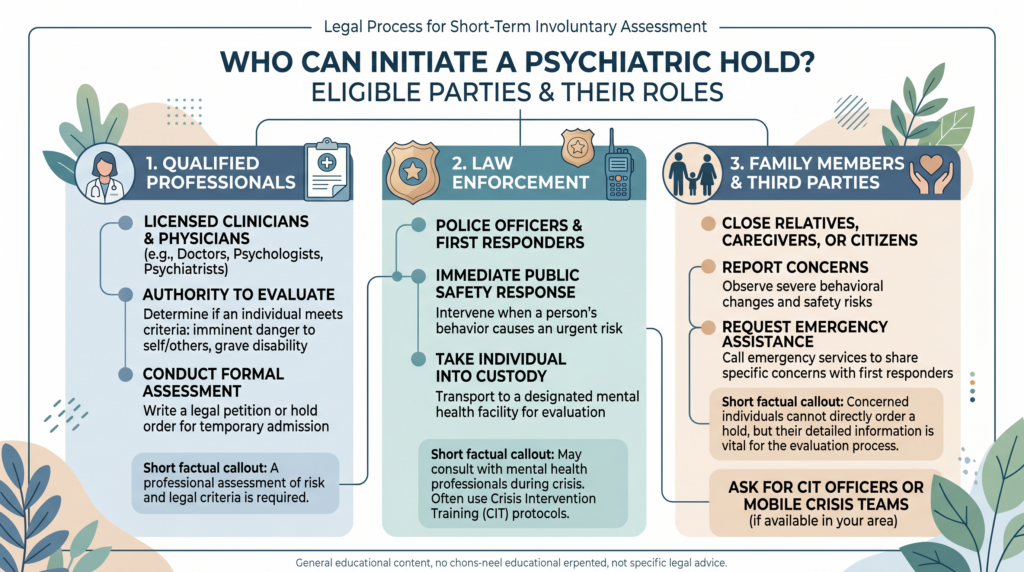
Who Can Initiate A Psychiatric Hold
Families often think they can “sign someone in.” In most places, that is not how it works.
Qualified Professionals
Psychiatrists, physicians, and in many states some licensed mental health clinicians can start a hold. Crisis workers and mobile crisis teams may also be able to evaluate and initiate the process.
This path is often more clinically focused and less chaotic than a police response. If a mobile crisis team is available in your area, it can be a steadier option.
Law Enforcement
Police in every state can usually initiate an emergency psychiatric detention when the legal standard appears to be met. The quality of that experience can vary a lot.
That is why Crisis Intervention Team, or CIT, training matters. If you call 911 for a psychiatric crisis, ask if a CIT officer or mobile crisis team is available.
Family Members And Third Parties
Family members usually cannot directly place someone on a hold. What you can do is report what you are seeing so a qualified person can assess the situation.
In some states, family can ask a judge or magistrate for a court-ordered evaluation. In others, a written statement or affidavit about dangerous behavior can support the process.
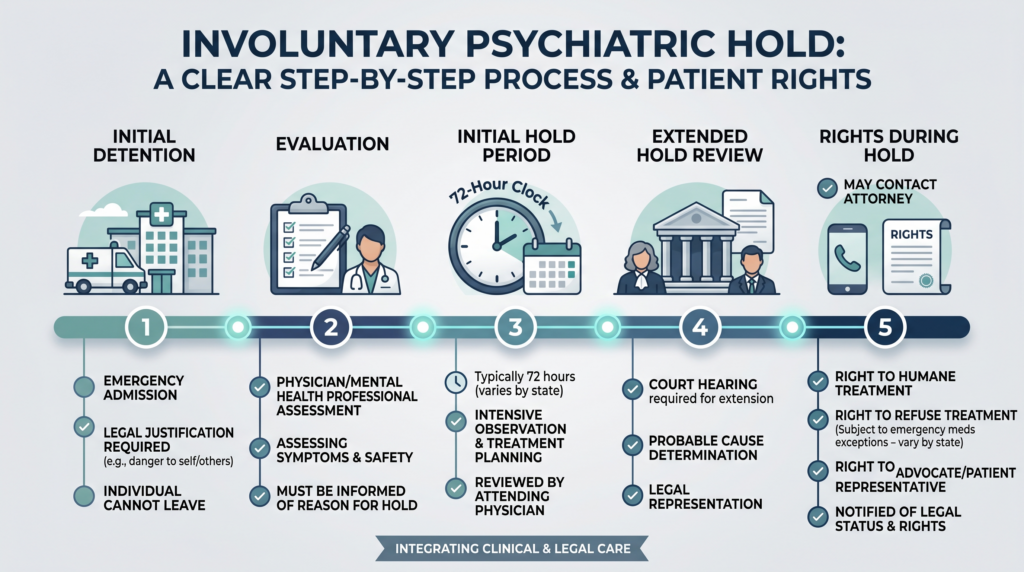
What Happens During The Hold: Step By Step
The process feels different depending on the state and the setting. Still, there is a rough pattern.
Initial Detention
The person is usually taken to an emergency room, psychiatric emergency service, or crisis stabilization unit. Transport may happen by ambulance, police, or sometimes by family if the person agrees to go and the situation is still safe.
Once the hold begins, the person cannot simply decide to leave. That loss of control is one reason the experience can feel so frightening.
Evaluation
A mental health professional evaluates whether the person meets the legal criteria to stay. This usually happens quickly, often within the first day.
If the evaluator decides the person does not meet criteria, they must be released. If the criteria are met, the hold continues for the allowed period under state law.
Initial Hold Period
In many states, the first hold lasts up to 72 hours. That does not always mean three full days in the unit.
The person may be observed, monitored, and given treatment aimed at acute stabilization. With bipolar disorder, that can mean managing agitation, severe insomnia, psychosis, suicidality, or dangerous impulsivity.
If A Longer Hold Is Needed
If the person still meets criteria when the first hold ends, the facility may seek a longer hold. That next step usually requires more legal process.
The name changes by state. In California, for example, a longer hold may be called a 5250.
At that stage, there is usually a hearing or review process. The person has the right to challenge the hold and to have representation.
Rights During An Involuntary Hold
A hold limits freedom, but it does not erase personhood. You still keep important rights.
Rights You Retain
You have the right to be told why you are being held. You also have the right to know what your rights are while you are there.
You generally have the right to contact an attorney and make a reasonable number of phone calls. You also have the right to appropriate treatment and to file a complaint with the facility.
Medication refusal is more complicated. In many states, you can refuse specific medications in some situations, but emergency medication can be given without consent during an acute safety crisis.
Rights That Are Temporarily Limited
You cannot leave during the hold period. That is the central limit.
Facilities may also restrict phone access, internet access, or outside communication for safety or clinical reasons. Those limits vary a lot by setting and state.
Confidentiality During A Hold
HIPAA still applies during an involuntary hold. Being on a hold does not cancel medical privacy laws.
What staff can tell your family depends on state law and on what permission you have given. In some states, the facility may notify family or next of kin that you are hospitalized, but detailed clinical information usually still needs your authorization.
For Family Members: What You Need To Know
When someone you love is in a bipolar crisis, your body knows it before your words do. Your chest tightens, your mind races, and every choice feels like it might break something.
How To Request A Hold For A Loved One
You usually cannot place the hold yourself. You can call 911 or 988 and report what is happening in clear, factual language.
Say what the person did, said, and had access to. “He said he will drive into traffic tonight and has his keys in his hand” is much more useful than “He’s acting crazy.”
If your loved one is willing to go voluntarily, taking them to a psychiatric ER can be simpler and less traumatic. If they are not willing and the danger is immediate, call emergency services.
Documenting The Crisis
Write things down. Dates, quotes, actions, access to weapons or medication, missed sleep, not eating, psychosis, threats, wandering, and recent attempts all matter.
Keep it factual and behavioral. “On Tuesday she had not slept for three nights, said she was chosen by God to jump off the balcony, and tried to climb the railing” gives a clinician something concrete to evaluate.
Some families use forms like California’s AB 1424 psychiatric history form. Even if your state uses a different tool, a written timeline can help police, ER staff, crisis teams, and courts understand what is actually happening.
During The Hold: What Family Can Do
You can ask staff if you may share collateral information with the treatment team. Even if they cannot tell you much, they may still be able to listen.
You can also ask about discharge planning. If the hold ends tomorrow, what comes next, who is prescribing medication, and where is follow-up happening?
What Not To Expect
A hold is not long-term bipolar treatment. It is a safety intervention during the worst part of the storm.
Your loved one may be furious with you afterward. That anger can be real and painful, even if the hold was necessary.
It may help to frame your actions plainly. You were scared for their safety, and you asked for help because the risk looked immediate.
How Bipolar Disorder Can Lead To A Hold
This part matters because self-knowledge comes before any plan. You need to know what your own brain looks like as it moves from strained to unsafe.
When bipolar symptoms escalate, the brain’s alarm, reward, and judgment systems can stop working together. In mania, the accelerator gets pinned down while the brakes wear thin, so a person may feel powerful, sleepless, invincible, and unable to see danger clearly.
In severe depression, the brain can narrow until the future disappears. That is when hopelessness can turn into suicidal planning, slowed thinking, and total collapse in self-care.
Psychosis makes all of this riskier. If you are hearing things, believing things that do not match reality, or acting on delusions, your ability to judge danger may be badly impaired.
This is why tracking early signs matters so much. Missed sleep, sudden spending, pressured speech, pacing, agitation, paranoia, withdrawal, giving things away, or talking like life is over can all be clues that a crisis is building.
If Treatment Begins During The Hold
Treatment sometimes starts right away. If it does, the right way to think about it is mechanism first, then evidence, then fit.
Sleep And Agitation Control
Mechanism: When mania or psychosis is driving the crisis, the brain is often stuck in an overactivated state with too much arousal and too little brake control. Medications used in the hospital often work by lowering that overactivation, reducing agitation, and helping the brain reconnect with sleep.
Evidence: In acute mania, antipsychotic medications and some mood stabilizers have strong evidence for reducing agitation, psychosis, and manic intensity over days to weeks. The most important caveat is that side effects differ a lot, so the exact medication choice matters.
Profile: These treatments tend to help people in severe mania, mixed states, psychosis, or dangerous insomnia where fast stabilization is the main goal. They are often used first in emergency settings because lack of sleep can pour gasoline on bipolar symptoms.
Mood Stabilizers
Mechanism: Mood stabilizers work by helping nerve signaling become less chaotic and less likely to swing into runaway highs or deep crashes. In plain English, they support steadier electrical and chemical signaling so the mood system is less jumpy over time.
Evidence: Several mood stabilizers have strong evidence for bipolar disorder, especially for preventing relapse and reducing manic symptoms. The main caveat is that some require blood monitoring and close dose adjustment.
Profile: These tend to fit people with recurrent mania, mixed episodes, or mood cycles that keep returning after the immediate crisis passes. They are usually part of longer-term management, not just the hold itself.
Therapy After Stabilization
Mechanism: Therapy helps the brain build prediction, pattern recognition, and safer responses before the next episode gains speed. It can turn scattered memories of a crisis into an actual map of triggers, warning signs, and next steps.
Evidence: Therapies designed for bipolar disorder, including psychoeducation, family-focused therapy, interpersonal and social rhythm therapy, and cognitive behavioral approaches, can reduce relapse risk when added to good medical care. The main caveat is that therapy works best once the person is stable enough to engage with it.
Profile: These approaches tend to help people who want better insight into triggers, sleep disruption, medication adherence, family conflict, and stress-related relapse. Family-focused work can be especially useful after a hold strained trust at home.
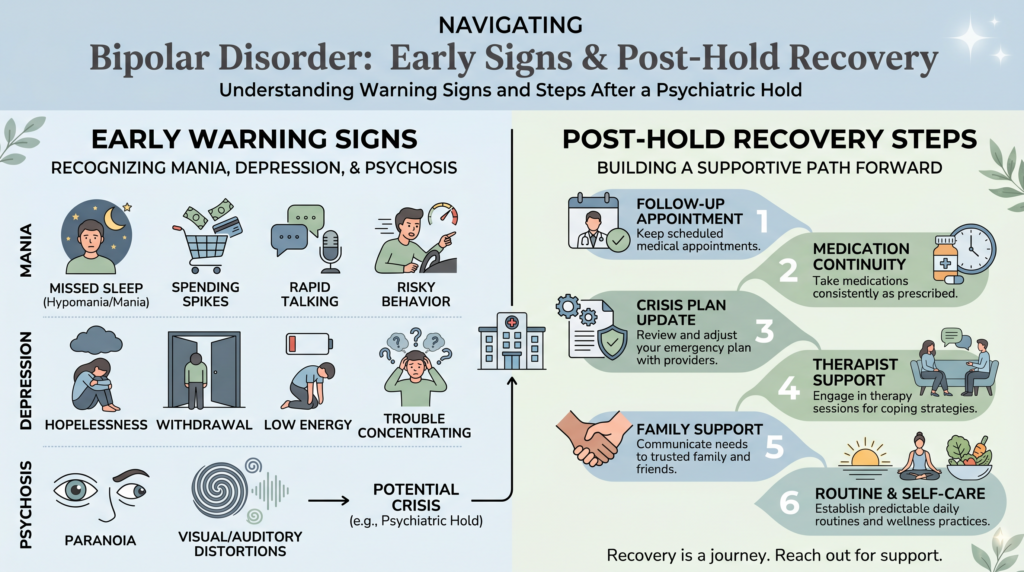
After The Hold: What Comes Next
The most dangerous part is not always the ambulance ride or the locked door. Sometimes it is the day after discharge, when everyone is wrung out and the follow-up plan is still blurry.
The Critical Transition
This period carries real risk. Appointments need to be lined up before discharge if possible.
Medication continuity matters a lot. If a person leaves with no bridge prescription, no pharmacy plan, or no next appointment, the odds of relapse rise fast.
For The Person Who Was Held
You may feel fear, shame, anger, relief, or all four before lunch. That mix is common.
Some people experience an involuntary hold as traumatic. Others believe it saved their life.
Both things can be true across different people, and sometimes inside the same person. Processing the experience with a therapist can help you sort memory from meaning and crisis from identity.
Once the dust settles, review the lead-up. What changed in your sleep, your speech, your spending, your beliefs, your energy, your appetite, and your sense of danger?
That review becomes your next crisis plan. It should include early warning signs, medications, emergency contacts, preferred hospitals, and what you want people to say or avoid saying when your brain starts slipping.
For Family Members
You may replay every moment and wonder if you overreacted or waited too long. That kind of guilt is common after a psychiatric crisis.
You need support too. NAMI family groups, peer groups, and individual therapy can help you recover from the fear and the moral weight of the experience.
The relationship may be strained for a while. Once your loved one is stable, family or couples therapy can help rebuild trust and make a better plan for next time.
State Laws Vary: How To Find Your State’s Rules
State law controls a lot of this. Names, timelines, medication rules, hearing rights, and family notification rules can all differ.
A good starting point is your state’s department of mental health website. You can also look at NAMI at nami.org, the Treatment Advocacy Center at treatmentadvocacycenter.org, or call the NAMI HelpLine at 1-800-950-6264 for state-specific guidance.
If you are in an active crisis now, call 988 in the United States. If there is immediate danger, call 911 and ask for a CIT officer if one is available.
Charting Your Next Baseline
A psychiatric hold is one of those lines in life that people remember in body detail. The fluorescent lights, the locked door, the paper bracelet, the phone call you never wanted to make.
Still, knowing your rights and knowing the actual threshold for a hold can return a little oxygen to the room. It gives you something solid to hold onto when bipolar disorder is making everything feel fast, sharp, and out of control.
If you live with bipolar disorder, learn your own warning signs before the next crisis tries to name them for you. If you love someone with bipolar disorder, keep your language specific, your notes factual, and your goal clear: safety first, then steadier ground.